

Including pharmacists on consultant-led ward rounds: a prospective non-randomised controlled trial
- PMID: 21853822
- PMCID: PMC5873735
- DOI: 10.7861/clinmedicine.11-4-312
Including pharmacists on consultant-led ward rounds: a prospective non-randomised controlled trial
Abstract
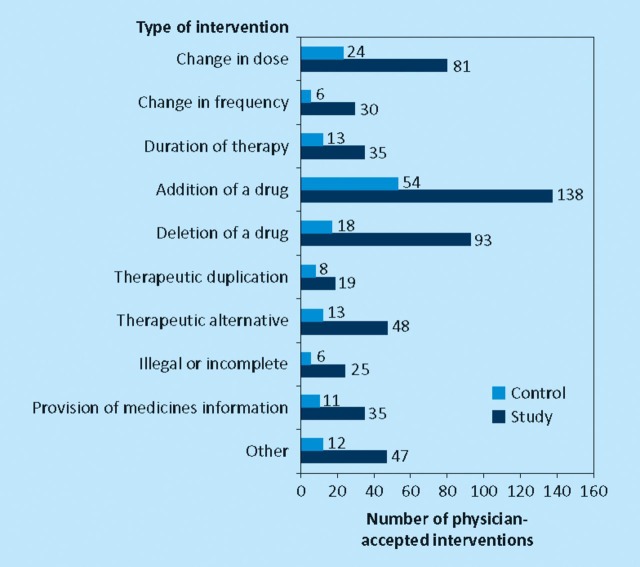
This study aimed to compare interventions made by pharmacists attending consultant-led ward rounds in addition to providing a ward pharmacy service, with those made by pharmacists providing a word pharmacy service alone. A prospective non-randomised controlled study on five inpatient medical wards was carried out at two teaching hospitals. A mean of 1.73 physician-accepted interventions were made per patient for the study group, compared to 0.89 for the control (Mann Whitney U, p < 0.001) with no difference between groups in the nature or clinical importance of the interventions. One physician-accepted intervention was made every eight minutes during the consultant-led ward rounds, compared to one every 63 minutes during a ward pharmacist visit. Pharmacists attending consultant-led ward rounds in addition to undertaking a ward pharmacist visit make significantly more interventions per patient than those made by pharmacists undertaking a ward pharmacist visit alone, rectifying prescribing errors and optimising treatment.
Comment in
-
Including pharmacists on consultant-led ward rounds.Clin Med (Lond). 2011 Dec;11(6):627-8; author reply 628. doi: 10.7861/clinmedicine.11-6-627. Clin Med (Lond). 2011. PMID: 22268327 Free PMC article. No abstract available.
References
-
- Stebbing C, Jacklin A, Barber N, Bates D. A comparison of the US and UK inpatient medication systems. Eur J Hosp Pharm Practice. 2006;12:36–40.
-
- Farrar K, Stoddart M, Slee A. Clinical pharmacy and reactive prescription review–time for a change? Pharm J. 1998;260:759–61.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
