

Extended antimicrobial treatment of bacterial vaginosis combined with human lactobacilli to find the best treatment and minimize the risk of relapses
- PMID: 21854593
- PMCID: PMC3176208
- DOI: 10.1186/1471-2334-11-223
Extended antimicrobial treatment of bacterial vaginosis combined with human lactobacilli to find the best treatment and minimize the risk of relapses
Abstract
Background: The primary objective of this study was to investigate if extended antibiotic treatment against bacterial vaginosis (BV) together with adjuvant lactobacilli treatment could cure BV and, furthermore, to investigate factors that could cause relapse.
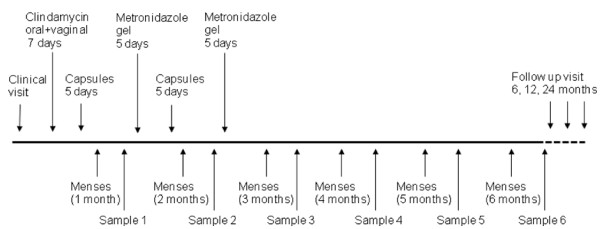
Methods: In all, 63 consecutive women with bacterial vaginosis diagnosed by Amsel criteria were offered a much more aggressive treatment of BV than used in normal clinical practice with repeated antibiotic treatment with clindamycin and metronidazole together with vaginal gelatine capsules containing different strains of lactobacilli both newly characterised and a commercial one (109 freeze-dried bacteria per capsule). Oral clindamycin treatment was also given to the patient's sexual partner.
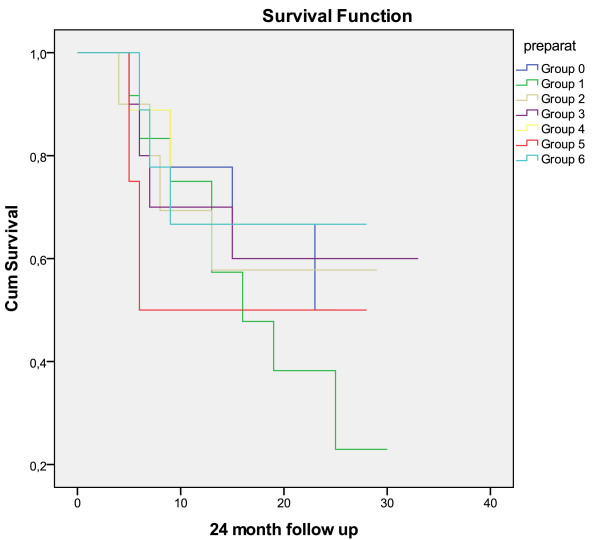
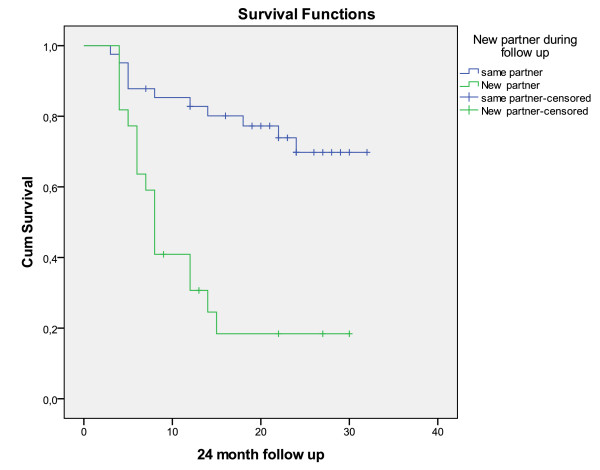
Results: The cure rate was 74.6% after 6 months. The patients were then followed as long as possible or until a relapse. The cure rate was 65.1% at 12 months and 55.6% after 24 months. There was no significant difference in cure rate depending on which Lactobacillus strains were given to the women or if the women were colonised by lactobacilli. The most striking factor was a new sex partner during the follow up period where the Odds Ratio of having a relapse was 9.3 (2.8-31.2) if the patients had a new sex partner during the observation period.
Conclusions: The study shows that aggressive treatment of the patient with antibiotics combined with specific Lactobacillus strain administration and partner treatment can provide long lasting cure. A striking result of our study is that change of partner is strongly associated with relapse of BV.
Trial registration: ClinicalTrials.gov: NCT01245322.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
