

High-resolution manometry studies are frequently imperfect but usually still interpretable
- PMID: 21854736
- PMCID: PMC3607365
- DOI: 10.1016/j.cgh.2011.08.007
High-resolution manometry studies are frequently imperfect but usually still interpretable
Abstract
Background & aims: Clinical esophageal manometry can be technically challenging. We investigated the prevalence and causes of technically imperfect, high-resolution esophageal pressure topography (EPT) studies at a tertiary referral hospital.
Methods: We reviewed 2000 consecutive clinical EPT studies that had been performed with consistent technique and protocol. A study was considered technically imperfect if there was a problem with pressure signal acquisition, if the catheter did not pass through the esophagogastric junction (EGJ), or if there were fewer than 7 evaluable swallows (without double-swallowing, and so forth). Data from the technically imperfect studies were interpreted blindly to determine a diagnosis; this diagnosis was compared with the diagnosis based on chart review.
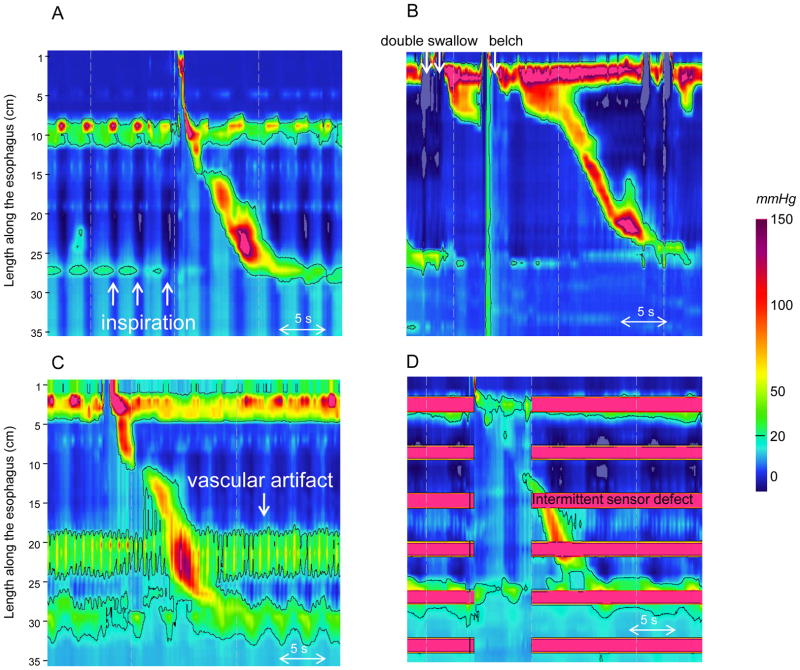
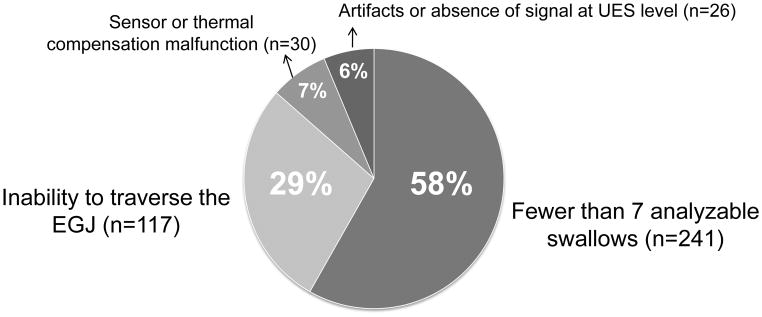
Results: We identified 414 technically imperfect studies (21% of the series). These were attributed to fewer than 7 evaluable swallows (58%), inability to traverse the EGJ (29%), sensor or thermal compensation malfunction (7%), and miscellaneous artifacts (6%). The most frequent causes of failure to traverse the EGJ were a large hiatal hernia (50%) and achalasia (24%). The condition most frequently associated with an incomplete swallow protocol was achalasia (33%). Despite the limitations, the diagnosis of achalasia was achieved correctly by blinded interpretation in 77% of cases and nonblinded interpretation in 94% of cases.
Conclusions: Technically imperfect EPT studies are common in a tertiary care center; large hiatal hernia and achalasia were the most frequent causes. However, despite the technical limitations, the data still could be interpreted, especially in the context of associated endoscopic and radiographic data.
Copyright © 2011 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Sabine Roman and John E. Pandolfino have served as consultant for Given Imaging.
Figures

Comment in
-
Making the most of imperfect high-resolution manometry studies.Clin Gastroenterol Hepatol. 2011 Dec;9(12):1015-6. doi: 10.1016/j.cgh.2011.09.024. Epub 2011 Oct 5. Clin Gastroenterol Hepatol. 2011. PMID: 21982965 No abstract available.
References
-
- Pandolfino JE, Kahrilas PJ American Gastroenterological A. American Gastroenterological Association medical position statement: Clinical use of esophageal manometry. Gastroenterology. 2005;128:207–208. - PubMed
-
- Murray JA, Clouse RE, Conklin JL. Components of the standard oesophageal manometry. Neurogastroenterol Motil. 2003;15:591–606. - PubMed
-
- Clouse RE, Staiano A, Alrakawi A, et al. Application of topographical methods to clinical esophageal manometry. Am J Gastroenterol. 2000;95:2720–2730. - PubMed
-
- Fox M, Hebbard G, Janiak P, et al. High-resolution manometry predicts the success of oesophageal bolus transport and identifies clinically important abnormalities not detected by conventional manometry. Neurogastroenterol Motil. 2004;16:533–542. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
