

Systematic review and meta-analysis of methotrexate use and risk of cardiovascular disease
- PMID: 21855836
- PMCID: PMC3196048
- DOI: 10.1016/j.amjcard.2011.06.054
Systematic review and meta-analysis of methotrexate use and risk of cardiovascular disease
Abstract
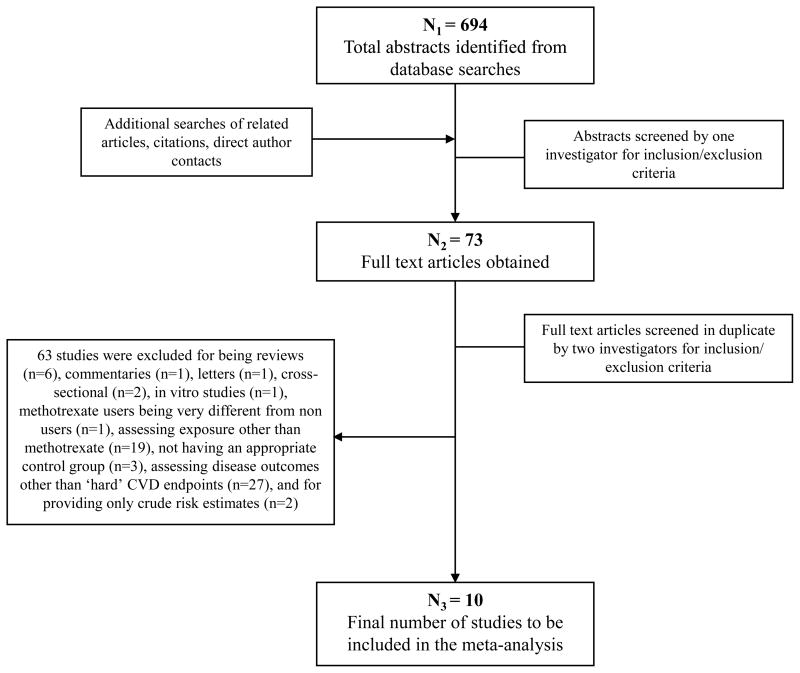
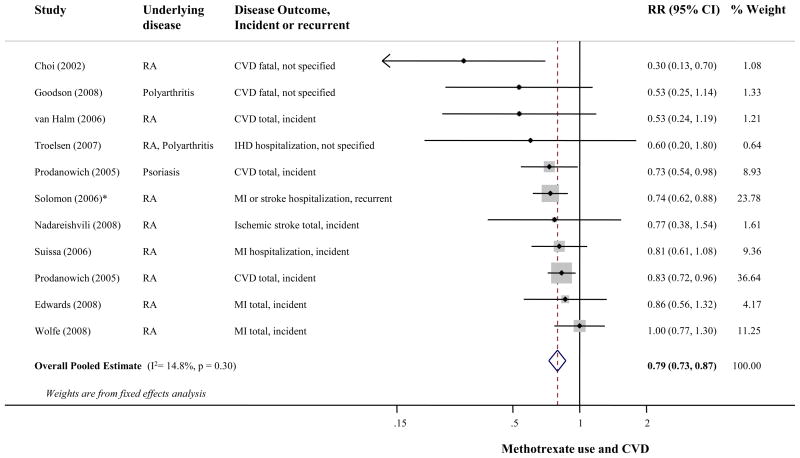
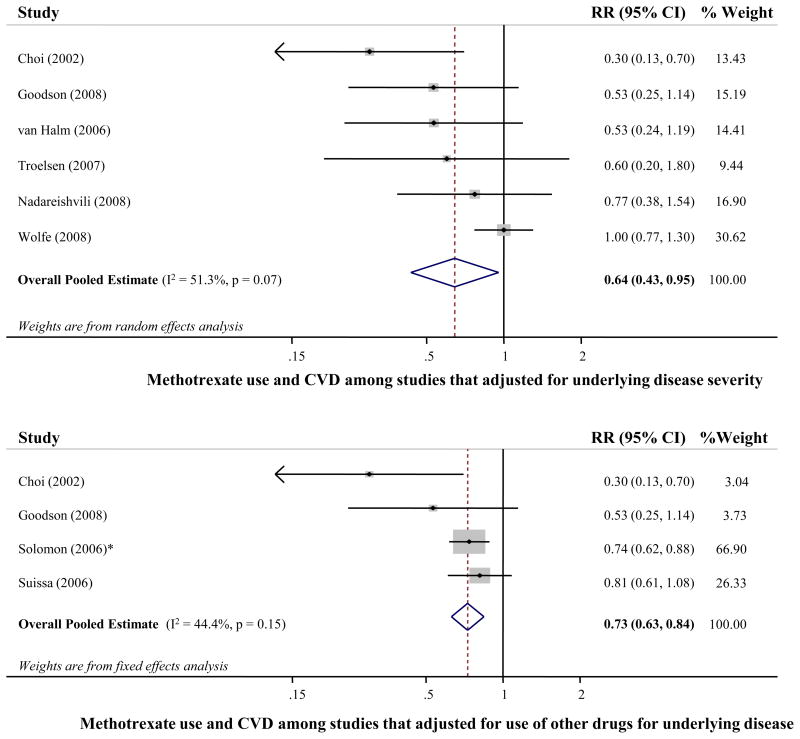
Inflammation predicts risk for cardiovascular disease (CVD) events, but the relation of drugs that directly target inflammation with CVD risk is not established. Methotrexate is a disease-modifying antirheumatic drug broadly used for the treatment of chronic inflammatory disorders. A systematic review and meta-analysis of evidence of relations of methotrexate with CVD occurrence were performed. Cohorts, case-control studies, and randomized trials were included if they reported associations between methotrexate and CVD risk. Inclusions and exclusions were independently adjudicated, and all data were extracted in duplicate. Pooled effects were calculated using inverse variance-weighted meta-analysis. Of 694 identified publications, 10 observational studies in which methotrexate was administered in patients with rheumatoid arthritis, psoriasis, or polyarthritis met the inclusion criteria. Methotrexate was associated with a 21% lower risk for total CVD (n = 10 studies, 95% confidence interval [CI] 0.73 to 0.87, p <0.001) and an 18% lower risk for myocardial infarction (n = 5, 95% CI 0.71 to 0.96, p = 0.01), without evidence for statistical between-study heterogeneity (p = 0.30 and p = 0.33, respectively). Among prespecified sources of heterogeneity explored, stronger associations were observed in studies that adjusted for underlying disease severity (relative risk 0.64, 95% CI 0.43 to 0.96, p <0.01) and for other concomitant medication (relative risk 0.73, 95% CI 0.63 to 0.84, p <0.001). Publication bias was potentially evident (funnel plot, Begg's test, p = 0.06); excluding studies with extreme risk estimates did not, however, alter results (relative risk 0.81, 95% CI 0.74 to 0.89). In conclusion, methotrexate use is associated with a lower risk for CVD in patients with chronic inflammation. These findings suggest that a direct treatment of inflammation may reduce CVD risk.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Methotrexate and risk of cardiovascular disease.Am J Cardiol. 2012 May 1;109(9):1383-4. doi: 10.1016/j.amjcard.2012.01.374. Am J Cardiol. 2012. PMID: 22500602 No abstract available.
References
-
- Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-Reactive Protein and Low-Density Lipoprotein Cholesterol Levels in the Prediction of First Cardiovascular Events. N Engl J Med. 2002;347:1557–1565. - PubMed
-
- Pai JK, Pischon T, Ma J, Manson JE, Hankinson SE, Joshipura K, Curhan GC, Rifai N, Cannuscio CC, Stampfer MJ, Rimm EB. Inflammatory Markers and the Risk of Coronary Heart Disease in Men and Women. N Engl J Med. 2004;351:2599–2610. - PubMed
-
- Cronstein BN. Low-Dose Methotrexate: A Mainstay in the Treatment of Rheumatoid Arthritis. Pharmacol Rev. 2005;57:163–172. - PubMed
-
- Westlake SL, Colebatch AN, Baird J, Kiely P, Quinn M, Choy E, Ostor AJK, Edwards CJ. The effect of methotrexate on cardiovascular disease in patients with rheumatoid arthritis: a systematic literature review. Rheumatology. 2010;49:295–307. - PubMed
-
- Ridker PM. Testing the inflammatory hypothesis of atherothrombosis: scientific rationale for the cardiovascular inflammation reduction trial (CIRT) J Thromb Haemost. 2009;7:332–339. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
