

Risk factors for astigmatism in preschool children: the multi-ethnic pediatric eye disease and Baltimore pediatric eye disease studies
- PMID: 21856010
- PMCID: PMC3186875
- DOI: 10.1016/j.ophtha.2011.06.031
Risk factors for astigmatism in preschool children: the multi-ethnic pediatric eye disease and Baltimore pediatric eye disease studies
Abstract
Objective: To evaluate risk factors for astigmatism in a population-based sample of preschool children.
Design: Population-based cross-sectional study.
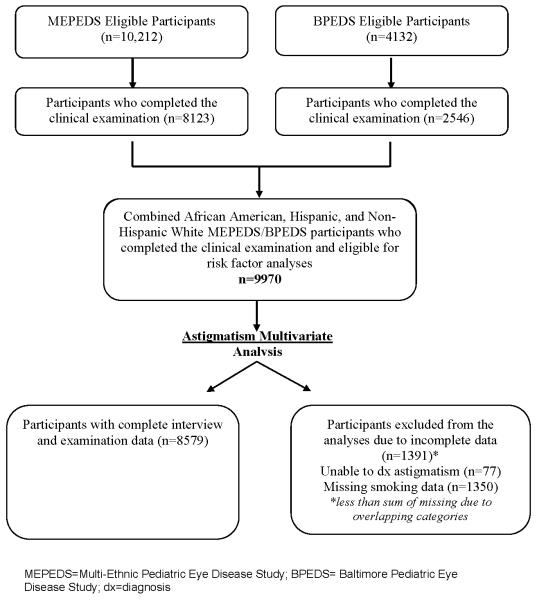
Participants: Population-based samples of 9970 children ages 6 to 72 months from Los Angeles County, California, and Baltimore, Maryland.
Methods: A cross-sectional study of children participating in the Multiethnic Pediatric Eye Disease Study and the Baltimore Eye Disease Study was completed. Data were obtained by clinical examination or by in-person interview. Odds ratios and 95% confidence intervals (CI) were calculated to evaluate potential associations between clinical, behavioral, or demographic factors and astigmatism.
Main outcome measures: Odds ratios (ORs) for various risk factors associated with astigmatism.
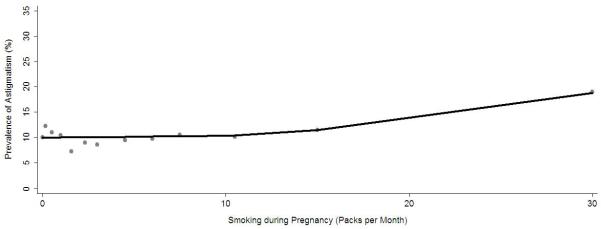
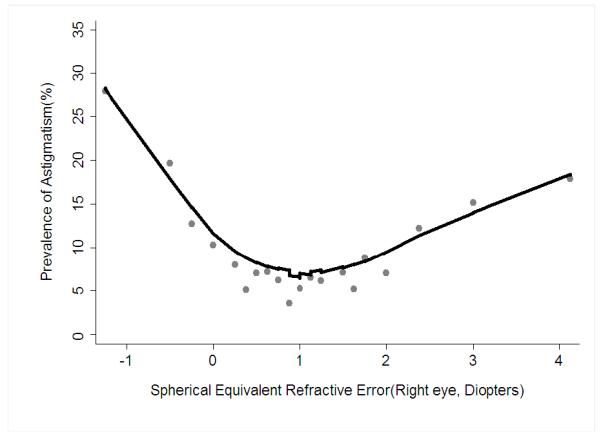
Results: Participants with myopia (≤-1.0 diopters) were 4.6 times as likely to have astigmatism (95% CI, 3.56-5.96) than those without refractive error, whereas participants with hyperopia (≥+2.00 diopters) were 1.6 times as likely (95% CI, 1.39-1.94). Children 6 to <12 months of age were approximately 3 times as likely to have astigmatism than children 5 to 6 years of age (95% CI, 2.28-3.73). Both Hispanic (OR, 2.38) and African-American (OR, 1.47) children were as likely to have astigmatism than non-Hispanic white children. Furthermore, children whose mothers smoked during pregnancy were 1.46 times (95% CI, 1.14-1.87) as likely to have astigmatism than children whose mothers did not smoke.
Conclusions: In addition to infancy, Hispanic and African-American race/ethnicity and correctable/modifiable risk factors such as myopia, hyperopia, and maternal smoking during pregnancy are associated with a higher risk of having astigmatism. Although the prevalence of smoking during pregnancy is typically low, this association may suggest etiologic pathways for future investigation.
Financial disclosure(s): The authors have no proprietary or commercial interest in any of the materials discussed in this article.
Copyright © 2011 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Amblyopia refractive risk factors.Ophthalmology. 2012 Jun;119(6):1283; author reply 1283-4. doi: 10.1016/j.ophtha.2012.02.011. Ophthalmology. 2012. PMID: 22656894 No abstract available.
References
-
- Porter J, Guirao A, Cox IG, Williams DR. Monochromatic aberrations of the human eye in a large population. J Opt Soc Am A Opt Image Sci Vis. 2001;18:1793–803. - PubMed
-
- Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom. 2007;90:5–19. - PubMed
-
- Abrahamsson M, Sjostrand J. Astigmatic axis and amblyopia in childhood. Acta Ophthalmol Scand. 2003;81:33–7. - PubMed
-
- Brown SA, Weih LM, Fu CL, et al. Prevalence of amblyopia and associated refractive errors in an adult population in Victoria, Australia. Ophthalmic Epidemiol. 2000;7:249–58. - PubMed
-
- Fulton AB, Hansen RM, Petersen RA. The relation of myopia and astigmatism in developing eyes. Ophthalmology. 1982;89:298–302. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
