

Comparative outcomes of tenofovir-based and zidovudine-based antiretroviral therapy regimens in Lusaka, Zambia
- PMID: 21857354
- PMCID: PMC3215810
- DOI: 10.1097/QAI.0b013e31823058a3
Comparative outcomes of tenofovir-based and zidovudine-based antiretroviral therapy regimens in Lusaka, Zambia
Abstract
Background: Although tenofovir (TDF) is a common component of antiretroviral therapy (ART), recent evidence suggests inferior outcomes when it is combined with nevirapine (NVP).
Methods: We compared outcomes among patients initiating TDF + emtricitabine or lamivudine (XTC) + NVP, TDF + XTC + efavirenz (EFV), zidovudine (ZDV) + lamuvidine (3TC) + NVP, and ZDV + 3TC + EFV. We categorized drug exposure by initial ART dispensation by a time-varying analysis that accounted for drug substitutions and by predominant exposure (>75% of drug dispensations) during an initial window period. Risks for death and program failure were estimated using Cox proportional hazard models. All regimens were compared with ZDV + 3TC + NVP.
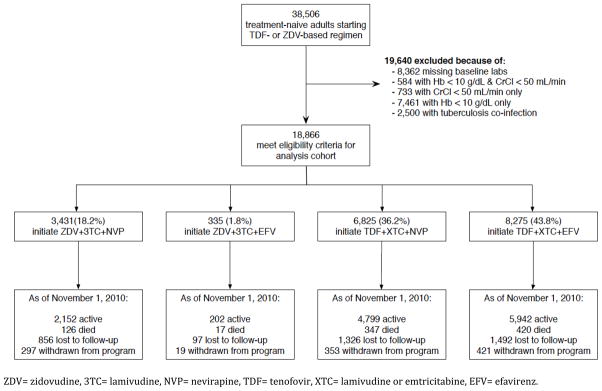
Results: Between July 2007 and November 2010, 18,866 treatment-naive adults initiated ART: 18.2% on ZDV + 3TC + NVP, 1.8% on ZDV + 3TC + EFV, 36.2% on TDF + XTC + NVP, and 43.8% on TDF + XTC + EFV. When exposure was categorized by initial prescription, patients on TDF + XTC + NVP [adjusted hazard ratio (AHR): 1.45; 95% confidence interval (CI): 1.03 to 2.06] had a higher post-90-day mortality. TDF + XTC + NVP was also associated with an elevated risk for mortality when exposure was categorized as time-varying (AHR: 1.51; 95% CI: 1.18 to 1.95) or by predominant exposure over the first 90 days (AHR: 1.91, 95% CI: 1.09 to 3.34). However, these findings were not consistently observed across sensitivity analyses or when program failure was used as a secondary outcome.
Conclusion: TDF + XTC + NVP was associated with higher mortality when compared with ZDV + 3TC + NVP but not consistently across sensitivity analyses. These findings may be explained in part by inherent limitations to our retrospective approach, including residual confounding. Further research is urgently needed to compare the effectiveness of ART regimens in use in resource-constrained settings.
Conflict of interest statement
Figures
References
-
- Gallant JE, DeJesus E, Arribas JR, et al. Tenofovir DF, emtricitabine, and efavirenz vs. zidovudine, lamivudine, and efavirenz for HIV. N Engl J Med. 2006;354:251–260. - PubMed
-
- Gallant JE, Staszewski S, Pozniak AL, et al. Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral-naive patients: a 3-year randomized trial. JAMA. 2004;292:191–201. - PubMed
-
- Margot NA, Isaacson E, McGowan I, Cheng A, Miller MD. Extended treatment with tenofovir disoproxil fumarate in treatment-experienced HIV-1-infected patients: genotypic, phenotypic, and rebound analyses. J Acquir Immune Defic Syndr. 2003;33:15–21. - PubMed
-
- Nelson MR, Katlama C, Montaner JS, et al. The safety of tenofovir disoproxil fumarate for the treatment of HIV infection in adults: the first 4 years. AIDS. 2007;21:1273–1281. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
