

Current concepts in the pathophysiology and management of hepatic encephalopathy
- PMID: 21857820
- PMCID: PMC3127024
Current concepts in the pathophysiology and management of hepatic encephalopathy
Abstract
Hepatic encephalopathy (HE) represents a broad continuum of neuropsychological dysfunction in patients with acute or chronic liver disease and/or portosystemic shunting of blood flow. The pathophysiology of this disease is quite complex, as it involves overproduction and reduced metabolism of various neurotoxins, particularly ammonia. Recent hypotheses implicate low-grade cerebral edema as a final common pathway for the pathophysiology of HE. Management of this condition is multifaceted and requires several steps: elimination of precipitating factors; removal of toxins, both by reducing them at their source and by augmenting scavenging pathways; modulation of resident fecal flora; proper nutritional support; and downregulation of systemic and gut-derived inflammation.
Keywords: Hepatic encephalopathy; ammonia; cerebral edema; glutaminase; urea cycle.
Figures
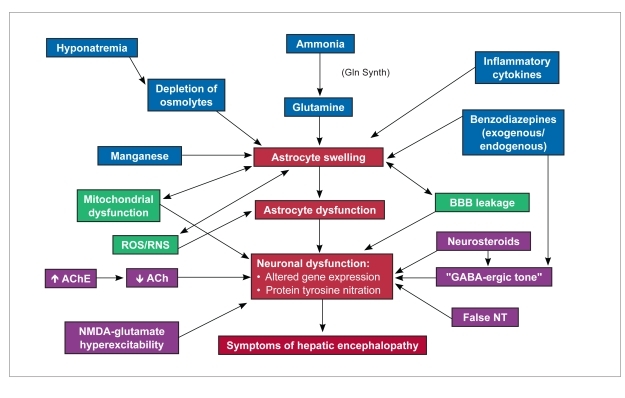
acetylcholine
acetylcholinesterase
blood brain barrier
gamma aminobutyric acid
glutamine synthetase
N-metyhl-D-aspartic acid
neurotransmitter
reactive nitrogen species
reactive oxygen species
References
-
- Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy—definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721. - PubMed
-
- Bajaj JS. Current and future diagnosis of hepatic encephalopathy. Metab Brain Dis. 2010;25:107–110. - PubMed
-
- Román E, Córdoba J, Torrens M, et al. Minimal hepatic encephalopathy is associated with falls. Am J Gastroenterol. 2011;106:476–482. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources