

Trabecular reorganization in consecutive iliac crest biopsies when switching from bisphosphonate to strontium ranelate treatment
- PMID: 21858188
- PMCID: PMC3156767
- DOI: 10.1371/journal.pone.0023638
Trabecular reorganization in consecutive iliac crest biopsies when switching from bisphosphonate to strontium ranelate treatment
Abstract
Background: Several agents are available to treat osteoporosis while addressing patient-specific medical needs. Individuals' residual risk to severe fracture may require changes in treatment strategy. Data at osseous cellular and microstructural levels due to a therapy switch between agents with different modes of action are rare. Our study on a series of five consecutively taken bone biopsies from an osteoporotic individual over a six-year period analyzes changes in cellular characteristics, bone microstructure and mineralization caused by a therapy switch from an antiresorptive (bisphosphonate) to a dual action bone agent (strontium ranelate).
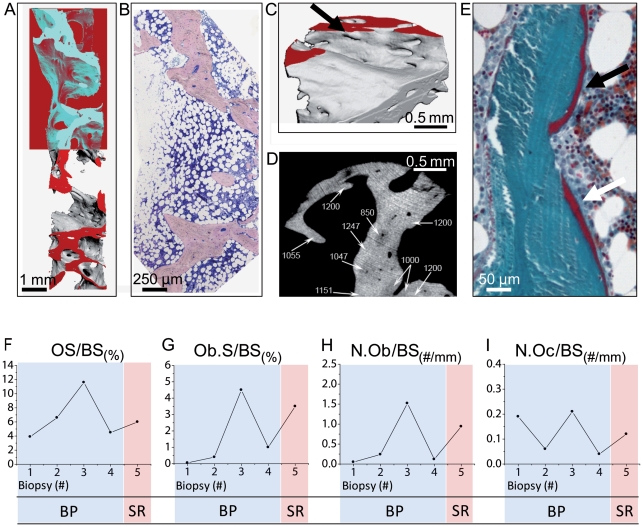
Methodology/principal findings: Biopsies were progressively taken from the iliac crest of a female patient. Four biopsies were taken during bisphosphonate therapy and one biopsy was taken after one year of strontium ranelate (SR) treatment. Furthermore, serum bone markers and dual x-ray absorptiometry measurements were acquired. Undecalcified histology was used to assess osteoid parameters and bone turnover. Structural indices and degree of mineralization were determined using microcomputed tomography, quantitative backscattered electron imaging, and combined energy dispersive x-ray/µ-x-ray-fluorescence microanalysis.
Conclusions/significance: Microstructural data revealed a notable increase in bone volume fraction after one year of SR treatment compared to the bisphosphonate treatment period. Indices of connectivity density, structure model index and trabecular bone pattern factor were predominantly enhanced indicating that the architectural transformation from trabecular rods to plates was responsible for the bone volume increase and less due to changes in trabecular thickness and number. Administration of SR following bisphosphonates led to a maintained mineralization profile with an uptake of strontium on the bone surface level. Reactivated osteoclasts designed tunneling, hook-like intratrabecular resorption sites. The appearance of tunneling resorption lacunae and the formation of both mini-modeling units and osteon-like structures within increased plate-like cancellous bone mass provides additional information on the mechanisms of strontium ranelate following bisphosphonate treatment, which may deserve special attention when monitoring a treatment switch.
Conflict of interest statement
Figures




Similar articles
-
Effects of strontium ranelate administration on bisphosphonate-altered hydroxyapatite: Matrix incorporation of strontium is accompanied by changes in mineralization and microstructure.Acta Biomater. 2010 Dec;6(12):4513-21. doi: 10.1016/j.actbio.2010.07.019. Epub 2010 Jul 21. Acta Biomater. 2010. PMID: 20654744 Clinical Trial.
-
In osteoporotic women treated with strontium ranelate, strontium is located in bone formed during treatment with a maintained degree of mineralization.Osteoporos Int. 2010 Apr;21(4):667-77. doi: 10.1007/s00198-009-1005-z. Epub 2009 Jul 14. Osteoporos Int. 2010. PMID: 19597910 Clinical Trial.
-
Distribution of strontium and mineralization in iliac bone biopsies from osteoporotic women treated long-term with strontium ranelate.Eur J Endocrinol. 2011 Sep;165(3):469-76. doi: 10.1530/EJE-11-0415. Epub 2011 Jun 20. Eur J Endocrinol. 2011. PMID: 21690207 Clinical Trial.
-
Strontium ranelate in osteoporosis.Curr Pharm Des. 2002;8(21):1907-16. doi: 10.2174/1381612023393639. Curr Pharm Des. 2002. PMID: 12171530 Review.
-
Strontium ranelate: a new paradigm in the treatment of osteoporosis.Drugs Today (Barc). 2003 Feb;39(2):89-101. doi: 10.1358/dot.2003.39.2.799416. Drugs Today (Barc). 2003. PMID: 12698204 Review.
Cited by
-
Guidelines for the assessment of bone density and microarchitecture in vivo using high-resolution peripheral quantitative computed tomography.Osteoporos Int. 2020 Sep;31(9):1607-1627. doi: 10.1007/s00198-020-05438-5. Epub 2020 May 26. Osteoporos Int. 2020. PMID: 32458029 Free PMC article.
-
Increased mechanical loading through controlled swimming exercise induces bone formation and mineralization in adult zebrafish.Sci Rep. 2018 Feb 26;8(1):3646. doi: 10.1038/s41598-018-21776-1. Sci Rep. 2018. PMID: 29483529 Free PMC article.
-
A holistic hip fracture approach: individualized diagnosis and treatment after surgery.Eur J Trauma Emerg Surg. 2014 Jun;40(3):265-71. doi: 10.1007/s00068-014-0374-y. Epub 2014 Jan 31. Eur J Trauma Emerg Surg. 2014. PMID: 26816059
-
A physiologically based pharmacokinetic model for strontium exposure in rat.Pharm Res. 2013 Jun;30(6):1536-52. doi: 10.1007/s11095-013-0991-x. Epub 2013 Mar 30. Pharm Res. 2013. PMID: 23543304
-
Role of Calcitonin and Strontium Ranelate in Osteoporosis.Indian J Orthop. 2023 Dec 4;57(Suppl 1):115-119. doi: 10.1007/s43465-023-01034-x. eCollection 2023 Dec. Indian J Orthop. 2023. PMID: 38107820 Free PMC article.
References
-
- Torgerson DJ, Bell-Syer SE. Hormone replacement therapy and prevention of nonvertebral fractures: a meta-analysis of randomized trials. JAMA. 2001;285:2891–2897. - PubMed
-
- Bilezikian JP. Efficacy of bisphosphonates in reducing fracture risk in postmenopausal osteoporosis. Am J Med. 2009;122:S14–21. - PubMed
-
- Ensrud KE, Stock JL, Barrett-Connor E, Grady D, Mosca L, et al. Effects of raloxifene on fracture risk in postmenopausal women: the Raloxifene Use for the Heart Trial. J Bone Miner Res. 2008;23:112–120. - PubMed
-
- Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344:1434–1441. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
