

Treatment of recurrent diffuse intrinsic pontine glioma: the MD Anderson Cancer Center experience
- PMID: 21858608
- PMCID: PMC3990187
- DOI: 10.1007/s11060-011-0677-3
Treatment of recurrent diffuse intrinsic pontine glioma: the MD Anderson Cancer Center experience
Abstract
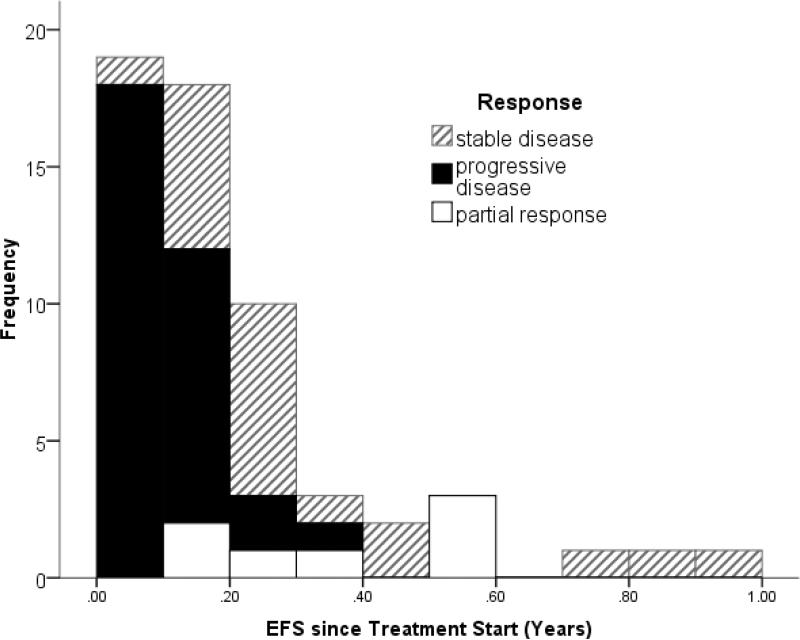
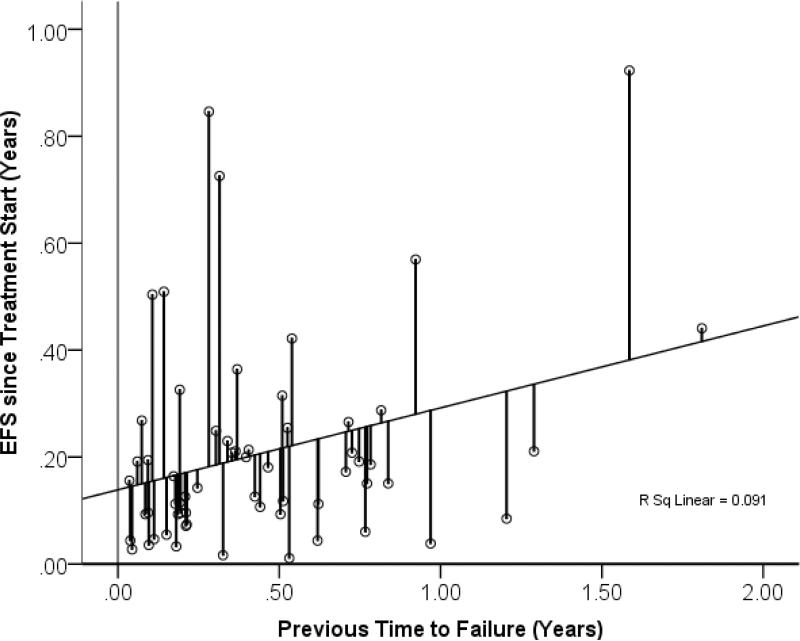
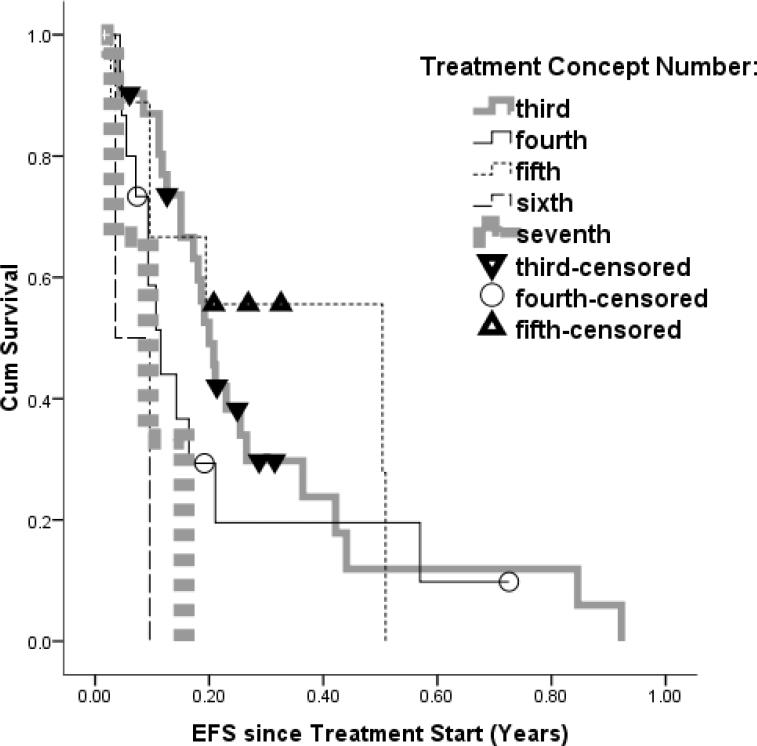
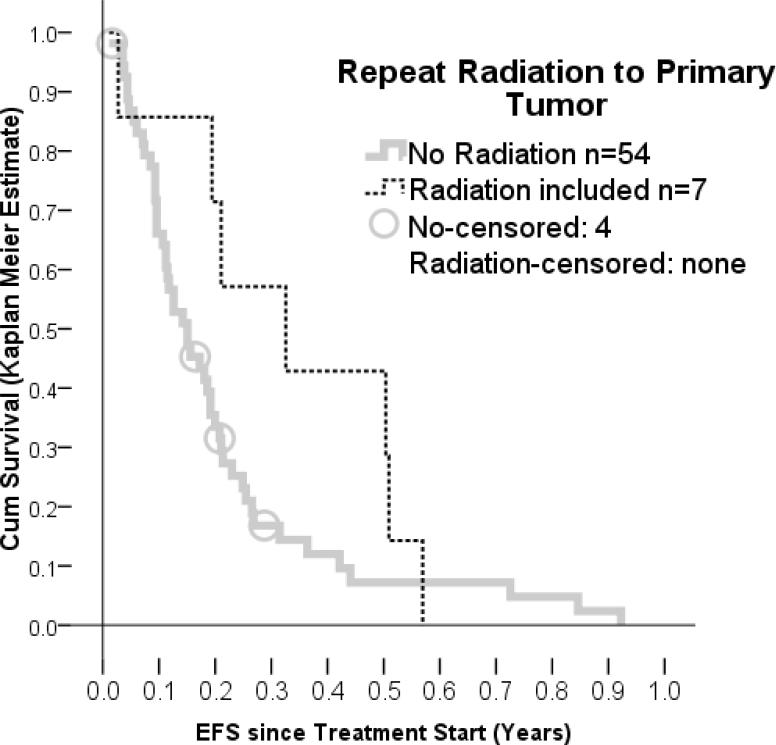
Recurrent diffuse intrinsic pontine gliomas (DIPG) are traditionally treated with palliative care since no effective treatments have been described for these tumors. Recently, clinical studies have been emerging, and individualized treatment is attempted more frequently. However, an informative way to compare the treatment outcomes has not been established, and historical control data are missing for recurrent disease. We conducted a retrospective chart review of patients with recurrent DIPG treated between 1998 and 2010. Response progression-free survival and possible influencing factors were evaluated. Thirty-one patients were identified who were treated in 61 treatment attempts using 26 treatment elements in 31 different regimens. The most frequently used drugs were etoposide (14), bevacizumab (13), irinotecan (13), nimotuzumab (13), and valproic acid (13). Seven patients had repeat radiation therapy to the primary tumor. Response was recorded after 58 treatment attempts and was comprised of 0 treatment attempts with complete responses, 7 with partial responses, 20 with stable diseases, and 31 with progressive diseases The median progression-free survival after treatment start was 0.16 years (2 months) and was found to be correlated to the prior time to progression but not to the number of previous treatment attempts. Repeat radiation resulted in the highest response rates (4/7), and the longest progression-free survival. These data provide a basis to plan future clinical trials for recurrent DIPG. Repeat radiation therapy should be tested in a prospective clinical study.
Figures
References
-
- Freeman CR, Krischer JP, Sanford RA, Cohen ME, Burger PC, del Carpio R, et al. Final results of a study of escalating doses of hyperfractionated radiotherapy in brain stem tumors in children: a Pediatric Oncology Group study. Int J Radiat Oncol Biol Phys. 1993;27(2):197–206. Available from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dop.... - PubMed
-
- Packer RJ, Boyett JM, Zimmerman RA, Rorke LB, Kaplan AM, Albright AL, et al. Hyperfractionated radiation therapy (72 Gy) for children with brain stem gliomas. A Childrens Cancer Group Phase I/II Trial. Cancer. 1993;72(4):1414–21. Available from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dop.... - PubMed
-
- Farmer JP, Montes JL, Freeman CR, Meagher-Villemure K, Bond MC, O'Gorman AM. Brainstem Gliomas. A 10-year institutional review. Pediatr Neurosurg. 2001;34(4):206–14. Available from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dop.... - PubMed
-
- Freeman CR, Farmer JP. Pediatric brain stem gliomas: a review. Int J Radiat Oncol Biol Phys. 1998;40(2):265–71. Available from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dop.... - PubMed
-
- Fangusaro J. Pediatric high-grade gliomas and diffuse intrinsic pontine gliomas. J Child Neurol. 2009;24(11):1409–17. Available from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dop.... - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
