

Tobacco smoking affects bacterial acquisition and colonization in oral biofilms
- PMID: 21859855
- PMCID: PMC3257914
- DOI: 10.1128/IAI.05371-11
Tobacco smoking affects bacterial acquisition and colonization in oral biofilms
Abstract
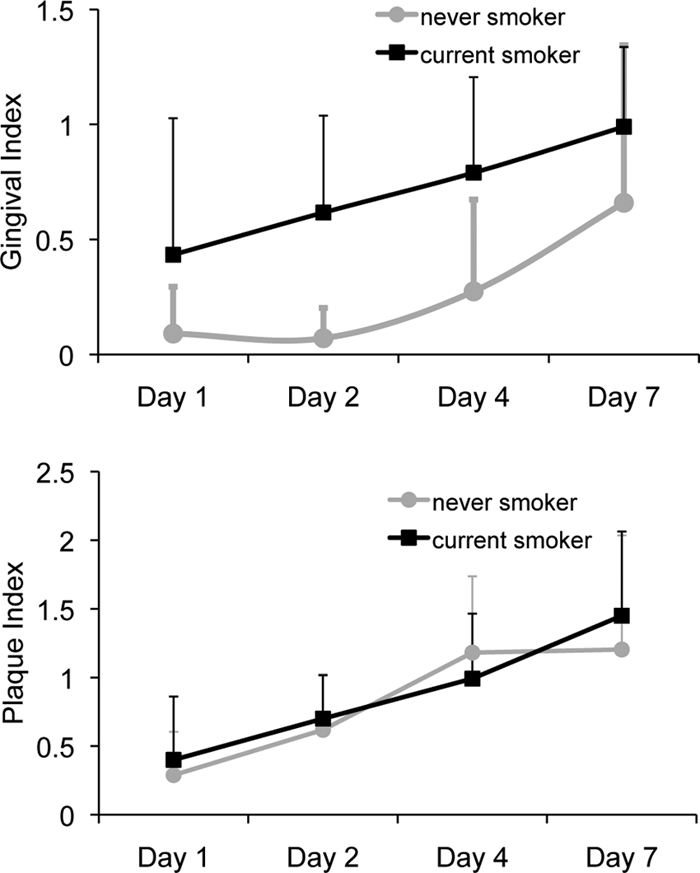
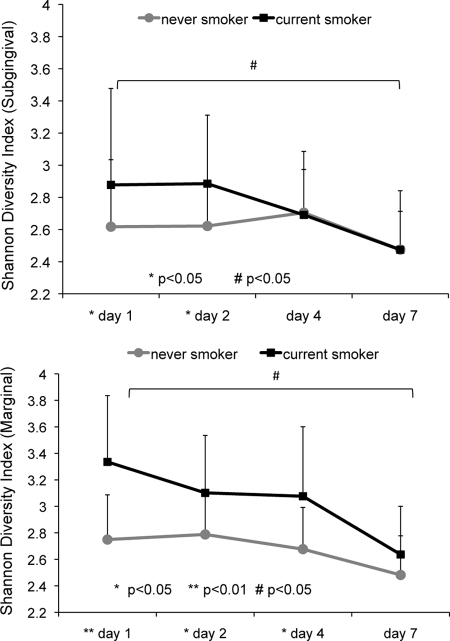
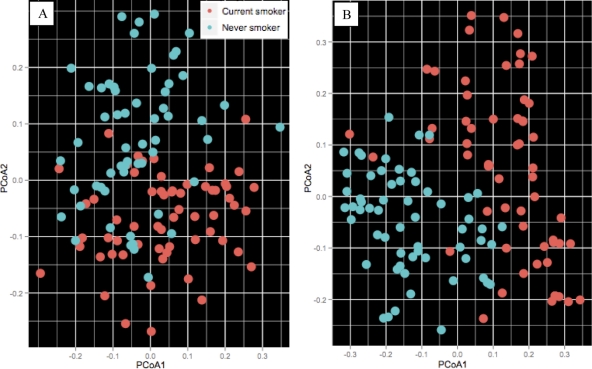
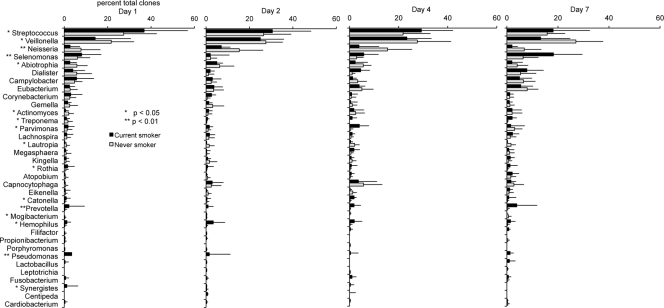
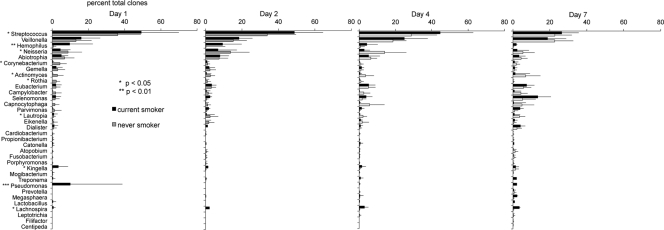
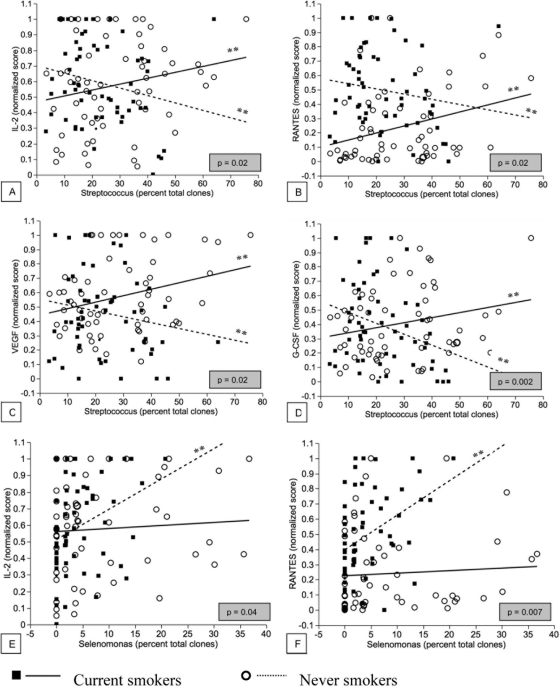
Recent evidence suggests that smoking affects the composition of the disease-associated subgingival biofilm, yet little is known about its effects during the formation of this biofilm. The present investigation was undertaken to examine the contributions of smoking to the composition and proinflammatory characteristics of the biofilm during de novo plaque formation. Marginal and subgingival plaque and gingival crevicular fluid samples were collected from 15 current smokers and from 15 individuals who had never smoked (nonsmokers) following 1, 2, 4, and 7 days of undisturbed plaque formation. 16S rRNA gene cloning and sequencing were used for bacterial identification, and multiplex bead-based flow cytometry was used to quantify the levels of 27 immune mediators. Smokers demonstrated a highly diverse, relatively unstable initial colonization of both marginal and subgingival biofilms, with lower niche saturation than that seen in nonsmokers. Periodontal pathogens belonging to the genera Fusobacterium, Cardiobacterium, Synergistes, and Selenomonas, as well as respiratory pathogens belonging to the genera Haemophilus and Pseudomonas, colonized the early biofilms of smokers and continued to persist over the observation period, suggesting that smoking favors early acquisition and colonization of pathogens in oral biofilms. Smokers also demonstrated an early proinflammatory response to this colonization, which persisted over 7 days. Further, a positive correlation between proinflammatory cytokine levels and commensal bacteria was observed in smokers but not in nonsmokers. Taken together, the data suggest that smoking influences both the composition of the nascent biofilm and the host response to this colonization.
Figures
References
-
- Ahijevych K. L., Wewers M. E. 1994. Patterns of cigarette consumption and cotinine levels among African American women smokers. Am. J. Respir. Crit. Care Med. 150:1229–1233 - PubMed
-
- Apatzidou D. A., Riggio M. P., Kinane D. F. 2005. Impact of smoking on the clinical, microbiological and immunological parameters of adult patients with periodontitis. J. Clin. Periodontol. 32:973–983 - PubMed
-
- Aronson M. D., Weiss S. T., Ben R. L., Komaroff A. L. 1982. Association between cigarette smoking and acute respiratory tract illness in young adults. JAMA 248:181–183 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
