

End points and outcomes in castration-resistant prostate cancer: from clinical trials to clinical practice
- PMID: 21859988
- PMCID: PMC3675708
- DOI: 10.1200/JCO.2011.35.8648
End points and outcomes in castration-resistant prostate cancer: from clinical trials to clinical practice
Abstract
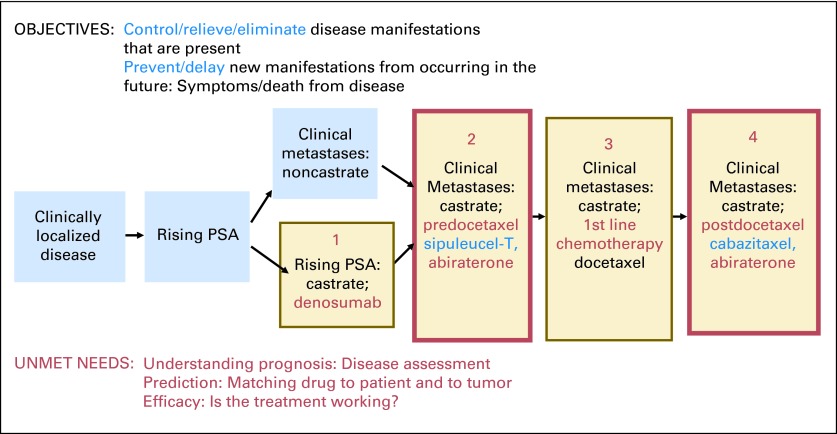
New therapeutic approaches for castration-resistant prostate cancer (CRPC) introduce new treatment dilemmas: how best to sequence these options to maximally benefit patients, what tests to perform before and after treatment to assess disease status, and how to interpret the test results and use them to guide treatment. New and specific end points for different classes of drugs are needed to provide the information to guide these treatment decisions. In 2008, the Prostate Cancer Working Group 2 consensus criteria for early-phase clinical trials redefined clinical trial end points as first, to control, relieve, or eliminate disease manifestations present when treatment is started and second, to prevent or delay future disease manifestations. Disease manifestations include prostate-specific antigen (PSA), soft-tissue disease (nodes and/or viscera), bone disease (most common site of spread), and symptoms. Recent US Food and Drug Administration (FDA) approvals for CRPC therapies have been based on the prevent/delay end points that reflect unequivocal benefit to a patient: prolongation of life or reduction in skeletal-related events (SREs). For the practicing oncologist, the control/relieve/eliminate outcomes should serve primarily to inform the decision of whether to continue therapy. In this review, we consider individual end points such as PSA, imaging, and patient-reported outcomes in the context of the control/relieve/eliminate and prevent/delay framework. We address the time-to-event end points of metastasis prevention, SRE, time to progression, and overall survival in the context of regulatory approvals. We also discuss circulating tumor cells measured with the CellSearch assay, recently cleared by the FDA for monitoring CRPC.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

References
-
- Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411–422. - PubMed
-
- de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet. 2010;376:1147–1154. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
