

Emerging therapies to prevent skeletal morbidity in men with prostate cancer
- PMID: 21860001
- PMCID: PMC3675709
- DOI: 10.1200/JCO.2010.34.4994
Emerging therapies to prevent skeletal morbidity in men with prostate cancer
Abstract
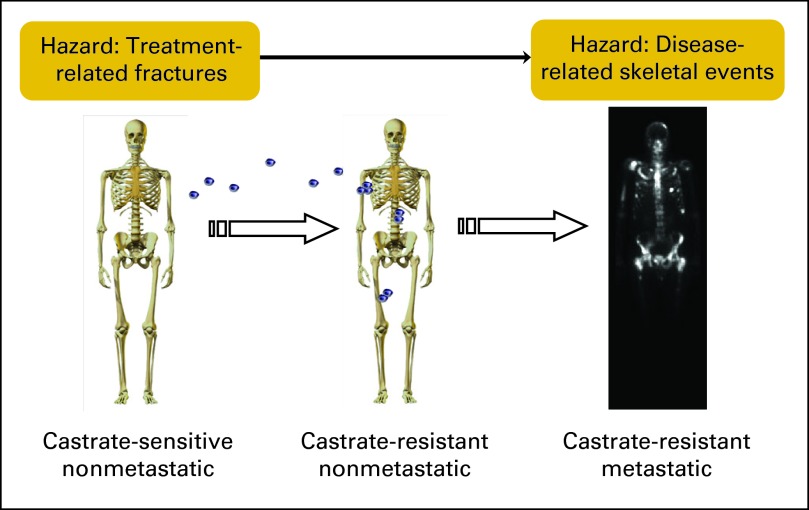
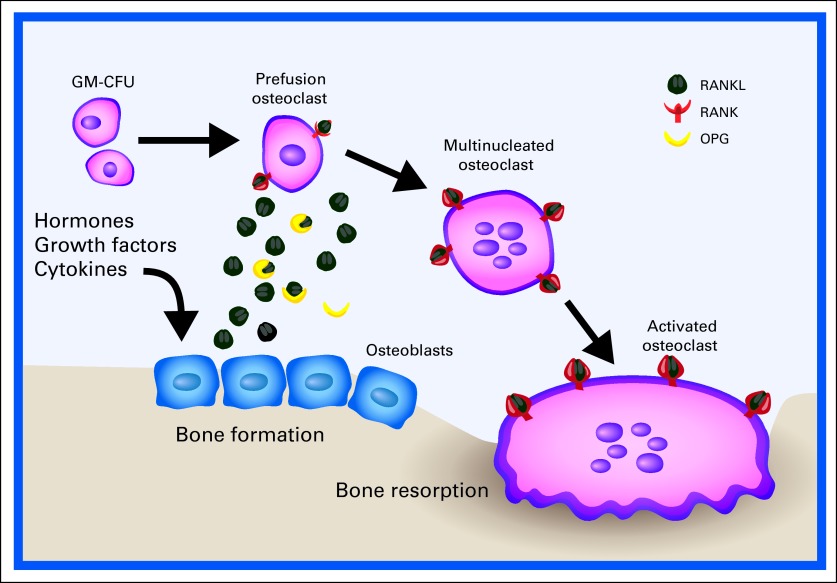
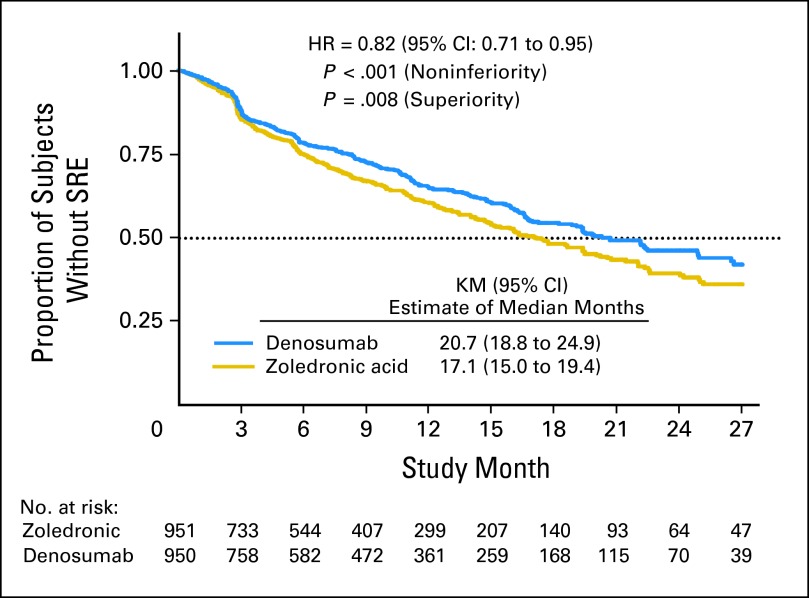
Skeletal morbidity is a prominent burden to men with advanced prostate cancer throughout the natural history of the disease. Bone metastases can cause pain and greatly elevate the risk for fractures and other structural complications. Distinct from the problem of metastases, treatment-related osteoporosis and associated fragility fractures are potential complications of androgen-deprivation therapy. Bone-targeted therapies for prostate cancer have therefore been the focus of considerable research and drug development efforts. The osteoclast is a validated therapeutic target in the management of prostate cancer. Osteoclast inhibition with zoledronic acid (a bisphosphonate) or with denosumab (a monoclonal antibody to RANK ligand) reduces risk for skeletal events in men with castration-resistant prostate cancer metastatic to bone. Osteoclast inhibition with any of several bisphosphonates improves bone mineral density, a surrogate for osteoporotic fracture risk. Denosumab and toremifene (a selective estrogen receptor modulator) have each been shown to reduce osteoporotic fracture risk among men receiving androgen-deprivation therapy. Beta-emitting radiopharmaceuticals reduce pain due to metastatic disease. Investigations involving alpha-emitting radium-223, endothelin-A receptor antagonists atrasentan and zibotentan, proto-oncogene tyrosine-protein kinase (SRC) inhibitor dasatinib, and tyrosine kinase inhibitor cabozantinib (XL184) are ongoing in clinical trials and are also discussed.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–1520. - PubMed
-
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. - PubMed
-
- Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int. 1997;7:407–413. - PubMed
-
- US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Office of the Surgeon General; 2004.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
