

Staphylococcal toxic shock syndrome 2000-2006: epidemiology, clinical features, and molecular characteristics
- PMID: 21860665
- PMCID: PMC3157910
- DOI: 10.1371/journal.pone.0022997
Staphylococcal toxic shock syndrome 2000-2006: epidemiology, clinical features, and molecular characteristics
Abstract
Introduction: Circulating strains of Staphylococcus aureus (SA) have changed in the last 30 years including the emergence of community-associated methicillin-resistant SA (MRSA). A report suggested staphylococcal toxic shock syndrome (TSS) was increasing over 2000-2003. The last population-based assessment of TSS was 1986.
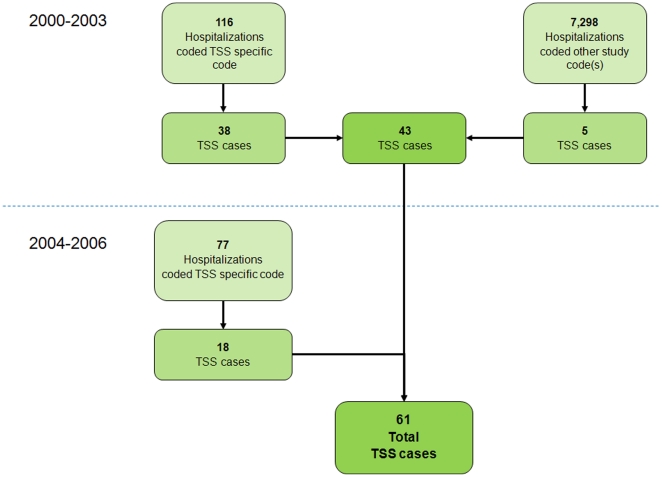
Methods: Population-based active surveillance for TSS meeting the CDC definition using ICD-9 codes was conducted in the Minneapolis-St. Paul area (population 2,642,056) from 2000-2006. Medical records of potential cases were reviewed for case criteria, antimicrobial susceptibility, risk factors, and outcome. Superantigen PCR testing and PFGE were performed on available isolates from probable and confirmed cases.
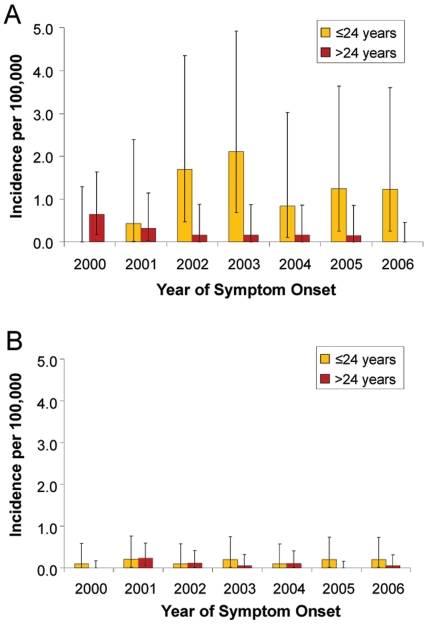
Results: Of 7,491 hospitalizations that received one of the ICD-9 study codes, 61 TSS cases (33 menstrual, 28 non-menstrual) were identified. The average annual incidence per 100,000 of all, menstrual, and non-menstrual TSS was 0.52 (95% CI, 0.32-0.77), 0.69 (0.39-1.16), and 0.32 (0.12-0.67), respectively. Women 13-24 years had the highest incidence at 1.41 (0.63-2.61). No increase in incidence was observed from 2000-2006. MRSA was isolated in 1 menstrual and 3 non-menstrual cases (7% of TSS cases); 1 isolate was USA400. The superantigen gene tst-1 was identified in 20 (80%) of isolates and was more common in menstrual compared to non-menstrual isolates (89% vs. 50%, p = 0.07). Superantigen genes sea, seb and sec were found more frequently among non-menstrual compared to menstrual isolates [100% vs 25% (p = 0.4), 60% vs 0% (p<0.01), and 25% vs 13% (p = 0.5), respectively].
Discussion: TSS incidence remained stable across our surveillance period of 2000-2006 and compared to past population-based estimates in the 1980s. MRSA accounted for a small percentage of TSS cases. tst-1 continues to be the superantigen associated with the majority of menstrual cases. The CDC case definition identifies the most severe cases and has been consistently used but likely results in a substantial underestimation of the total TSS disease burden.
Conflict of interest statement
Figures
References
-
- Stevens FA. The occurence of Staphylococcus aureus infection with a scarlitiniform rash. JAMA. 1927;88:1957–1958.
-
- Todd J, Fishaut M, Kapral F, Welch T. Toxic-shock syndrome associated with phage-group-I Staphylococci. Lancet. 1978;2:1116–1118. - PubMed
-
- Shands KN, Schmid GP, Dan BB, Blum D, Guidotti RJ, et al. Toxic-shock syndrome in menstruating women: association with tampon use and Staphylococcus aureus and clinical features in 52 cases. N Engl J Med. 1980;303:1436–1442. - PubMed
-
- Davis JP, Chesney PJ, Wand PJ, LaVenture M. Toxic-shock syndrome: epidemiologic features, recurrence, risk factors, and prevention. N Engl J Med. 1980;303:1429–1435. - PubMed
-
- Schlievert PM, Osterholm MT, Kelly JA, Nishimura RD. Toxin and enzyme characterization of Staphylococcus aureus isolates from patients with and without toxic shock syndrome. Ann Intern Med. 1982;96:937–940. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
