

Abdominal hernias: Radiological features
- PMID: 21860678
- PMCID: PMC3158902
- DOI: 10.4253/wjge.v3.i6.110
Abdominal hernias: Radiological features
Abstract
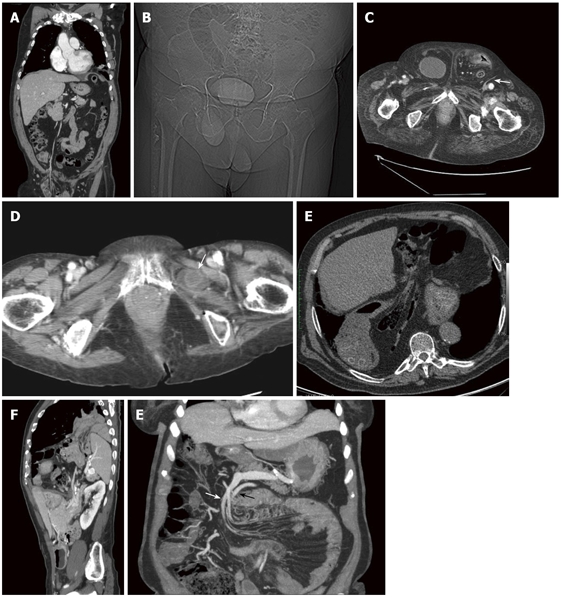
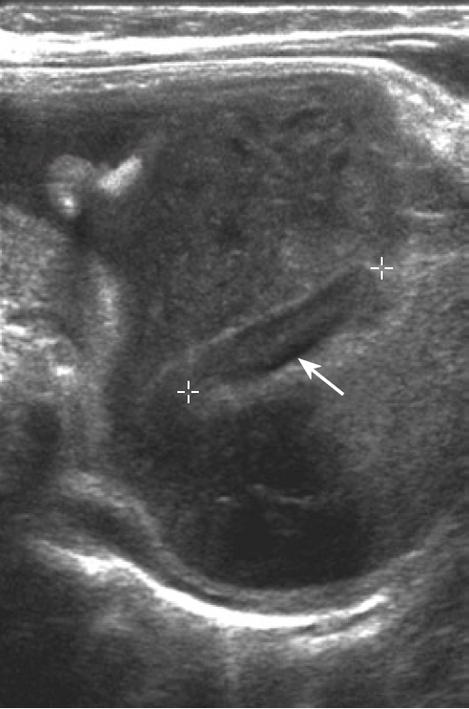
Abdominal wall hernias are common diseases of the abdomen with a global incidence approximately 4%-5%. They are distinguished in external, diaphragmatic and internal hernias on the basis of their localisation. Groin hernias are the most common with a prevalence of 75%, followed by femoral (15%) and umbilical (8%). There is a higher prevalence in males (M:F, 8:1). Diagnosis is usually made on physical examination. However, clinical diagnosis may be difficult, especially in patients with obesity, pain or abdominal wall scarring. In these cases, abdominal imaging may be the first clue to the correct diagnosis and to confirm suspected complications. Different imaging modalities are used: conventional radiographs or barium studies, ultrasonography and Computed Tomography. Imaging modalities can aid in the differential diagnosis of palpable abdominal wall masses and can help to define hernial contents such as fatty tissue, bowel, other organs or fluid. This work focuses on the main radiological findings of abdominal herniations.
Keywords: Abdominal Radiology; Abdominal Wall; Computed tomography; Diagnostic Radiology; External Hernia; Hernia; Hiatal Hernia; Internal Hernia; Intestinal Obstruction; Ultrasonography.
Figures

References
-
- Mathieu D, Luciani A. Internal abdominal herniations. AJR Am J Roentgenol. 2004;183:397–404. - PubMed
-
- Digestive diseases in the United States: Epidemiology and Impact. NIH Publication No. 94-1447. Bethesda: NIDDK; 1994.
-
- Aguirre DA, Casola G, Sirlin C. Abdominal wall hernias: MDCT findings. AJR Am J Roentgenol. 2004;183:681–690. - PubMed
-
- Rutkow IM. Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am. 2003;83:1045–151, 1045-151. - PubMed
-
- Madoz A, Franpas E, D’Alincourt A, Perret C, Laute F, Liebault B, Dupas B. Imagerie des hernies pariétale abdominales. Elsevier Masson SAS. 2007;33:A39.
LinkOut - more resources
Full Text Sources
Medical
