

Imaging and interventions in Budd-Chiari syndrome
- PMID: 21860712
- PMCID: PMC3158894
- DOI: 10.4329/wjr.v3.i7.169
Imaging and interventions in Budd-Chiari syndrome
Abstract
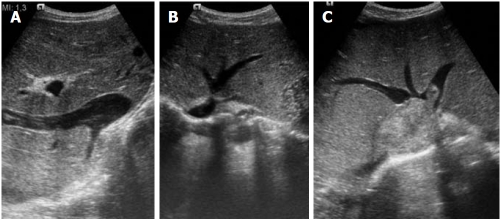
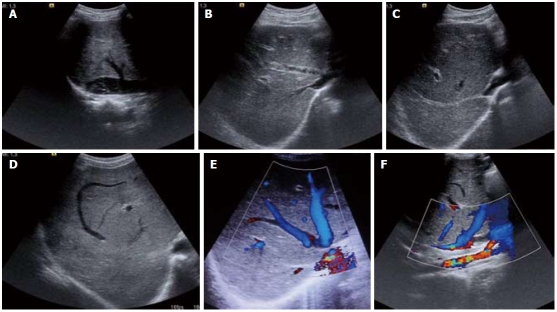
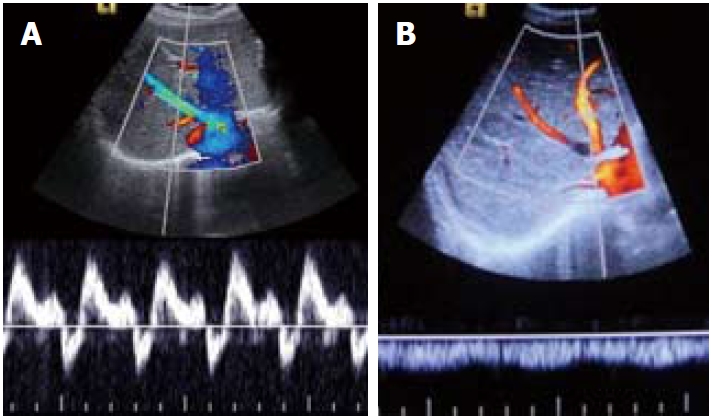
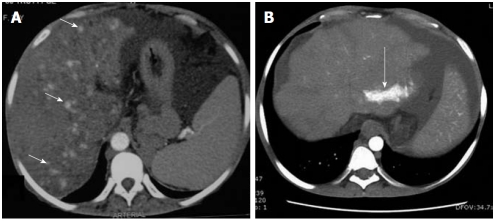
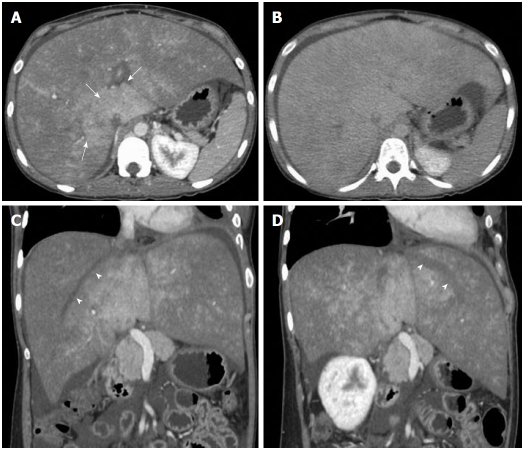
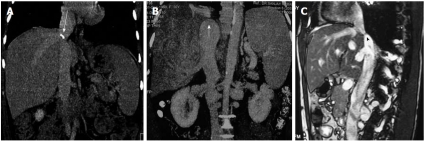
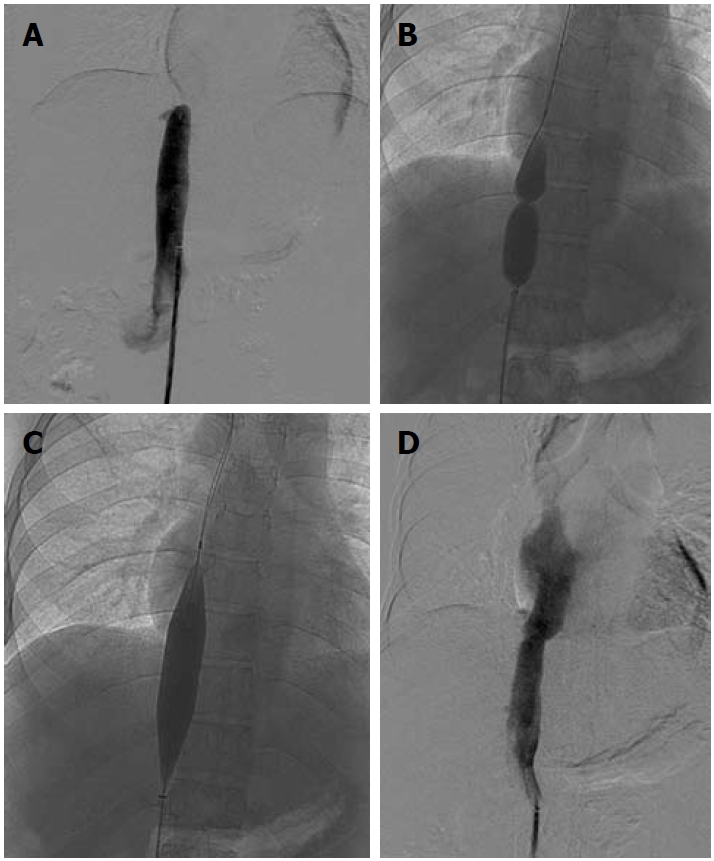
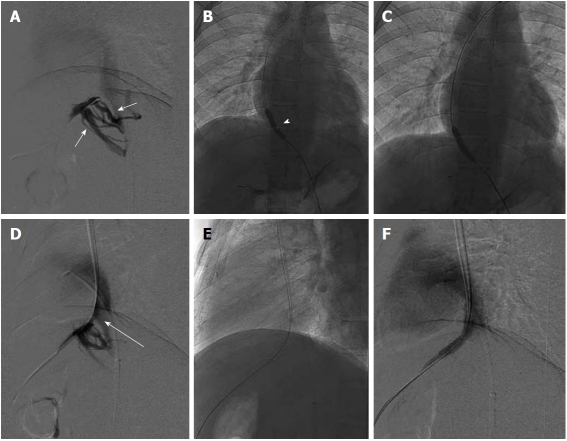
Budd-Chiari syndrome (BCS) consists of a group of disorders with obstruction of hepatic venous outflow leading to increased hepatic sinusoidal pressure and portal hypertension. Clinically, two forms of disease (acute and chronic) are recognized. Mostly the patients present with ascites, hepatomegaly, and portal hypertension. In acute disease the liver is enlarged with thrombosed hepatic veins (HV) and ascites, whereas in the chronic form of the disease there may be membranous occlusion of HV and/or the inferior vena cava (IVC), or there may be short or long segment fibrotic constriction of HV or the suprahepatic IVC. Due to advances in radiological interventional techniques and hardware, there have been changes in the management protocol of BCS with surgery being offered to patients not suitable for radiological interventions or having acute liver failure requiring liver transplantation. The present article gives an insight into various imaging findings and interventional techniques employed in the management of BCS.
Keywords: Budd-Chiari syndrome; Hepatic vein angioplasty/stenting; Inferior vena cava angioplasty; Transjugular intrahepatic portosystemic shunt.
Figures
Similar articles
-
Radiological interventions in HVOTO--practical tips.Trop Gastroenterol. 2011 Jan-Mar;32(1):4-14. Trop Gastroenterol. 2011. PMID: 21922850 Review.
-
Good Clinical Outcomes in Budd-Chiari Syndrome with Hepatic Vein Occlusion.Dig Dis Sci. 2016 Oct;61(10):3054-3060. doi: 10.1007/s10620-016-4208-0. Epub 2016 May 25. Dig Dis Sci. 2016. PMID: 27221497
-
Interventions in Budd-Chiari syndrome: an updated review.Abdom Radiol (NY). 2025 Mar;50(3):1307-1319. doi: 10.1007/s00261-024-04558-4. Epub 2024 Sep 26. Abdom Radiol (NY). 2025. PMID: 39325211 Review.
-
Budd-Chiari syndrome and extensive inferior vena cava thrombosis treated with sequential interventional radiology and transjugular intrahepatic portosystemic shunting: A case report from Kenya.SAGE Open Med Case Rep. 2023 Mar 21;11:2050313X231161190. doi: 10.1177/2050313X231161190. eCollection 2023. SAGE Open Med Case Rep. 2023. PMID: 36968991 Free PMC article.
-
Transjugular intrahepatic portosystemic shunt for severe jaundice in patients with acute Budd-Chiari syndrome.World J Gastroenterol. 2015 Feb 28;21(8):2413-8. doi: 10.3748/wjg.v21.i8.2413. World J Gastroenterol. 2015. PMID: 25741149 Free PMC article.
Cited by
-
Initial imaging analysis of Budd-Chiari syndrome in Henan province of China: most cases have combined inferior vena cava and hepatic veins involvement.PLoS One. 2014 Jan 8;9(1):e85135. doi: 10.1371/journal.pone.0085135. eCollection 2014. PLoS One. 2014. PMID: 24416352 Free PMC article.
-
Budd-Chiari syndrome: consensus guidance of the Asian Pacific Association for the study of the liver (APASL).Hepatol Int. 2021 Jun;15(3):531-567. doi: 10.1007/s12072-021-10189-4. Epub 2021 Jul 8. Hepatol Int. 2021. PMID: 34240318
-
Interventional Treatment of Budd-Chiari Syndrome.Diagnostics (Basel). 2023 Apr 18;13(8):1458. doi: 10.3390/diagnostics13081458. Diagnostics (Basel). 2023. PMID: 37189559 Free PMC article. Review.
-
Imaging Diagnosis of Splanchnic Venous Thrombosis.Gastroenterol Res Pract. 2015;2015:101029. doi: 10.1155/2015/101029. Epub 2015 Oct 12. Gastroenterol Res Pract. 2015. PMID: 26600801 Free PMC article. Review.
-
State of the Art, Current Perspectives, and Controversies of Budd-Chiari Syndrome: A Review.J Clin Med Res. 2022 Apr;14(4):147-157. doi: 10.14740/jocmr4724. Epub 2022 Apr 30. J Clin Med Res. 2022. PMID: 35573933 Free PMC article. Review.
References
-
- Ludwig J, Hashimoto E, McGill DB, van Heerden JA. Classification of hepatic venous outflow obstruction: ambiguous terminology of the Budd-Chiari syndrome. Mayo Clin Proc. 1990;65:51–55. - PubMed
-
- Hadengue A, Poliquin M, Vilgrain V, Belghiti J, Degott C, Erlinger S, Benhamou JP. The changing scene of hepatic vein thrombosis: recognition of asymptomatic cases. Gastroenterology. 1994;106:1042–1047. - PubMed
-
- Denninger MH, Chaït Y, Casadevall N, Hillaire S, Guillin MC, Bezeaud A, Erlinger S, Briere J, Valla D. Cause of portal or hepatic venous thrombosis in adults: the role of multiple concurrent factors. Hepatology. 2000;31:587–591. - PubMed
-
- Mohanty D, Shetty S, Ghosh K, Pawar A, Abraham P. Hereditary thrombophilia as a cause of Budd-Chiari syndrome: a study from Western India. Hepatology. 2001;34:666–670. - PubMed
-
- Valla D, Le MG, Poynard T, Zucman N, Rueff B, Benhamou JP. Risk of hepatic vein thrombosis in relation to recent use of oral contraceptives. A case-control study. Gastroenterology. 1986;90:807–811. - PubMed
LinkOut - more resources
Full Text Sources
