

Endovascular management in abdominal visceral arterial aneurysms: A pictorial essay
- PMID: 21860714
- PMCID: PMC3158896
- DOI: 10.4329/wjr.v3.i7.182
Endovascular management in abdominal visceral arterial aneurysms: A pictorial essay
Abstract
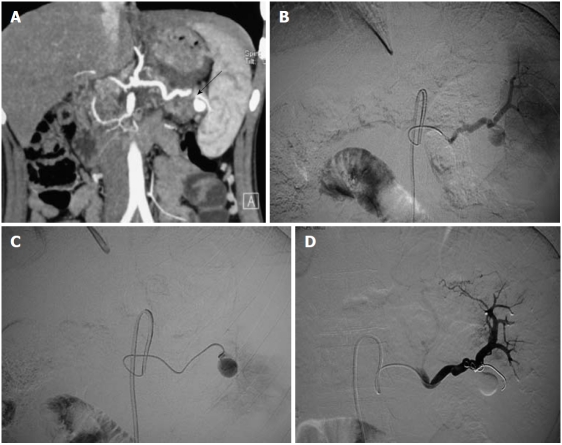
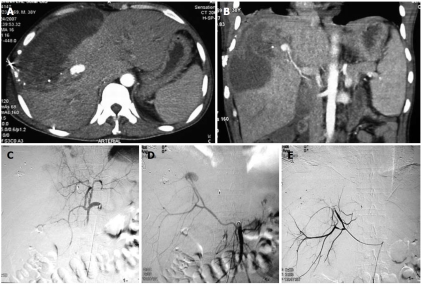
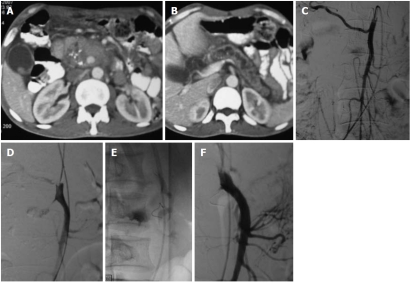
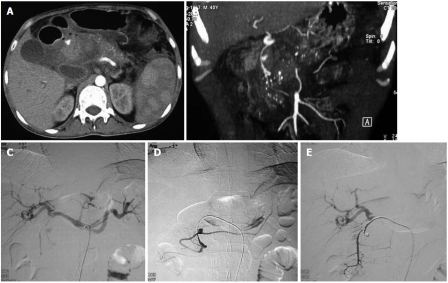
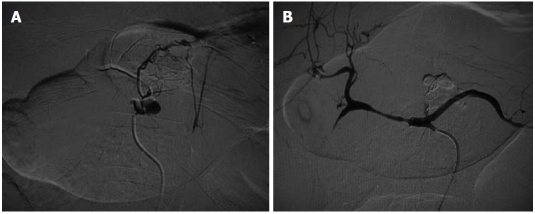
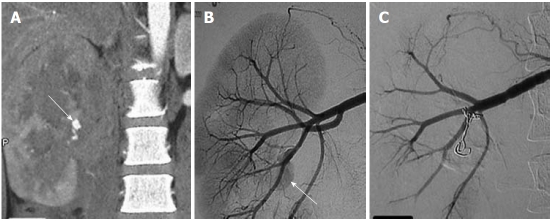
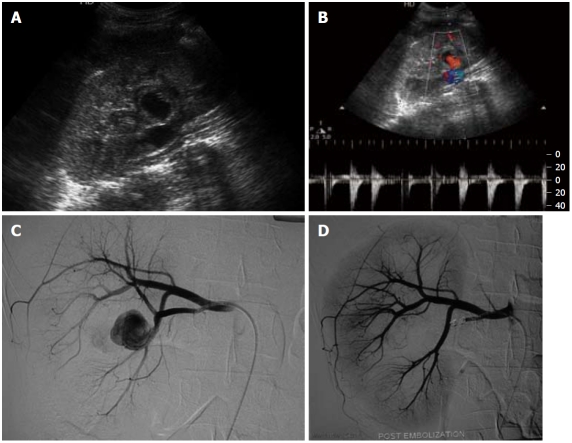
Visceral artery aneurysms (VAAs) include aneurysms of the splanchnic circulation and those of the renal artery. Their diagnosis is clinically important because of the associated high mortality and potential complications. Splenic, superior mesenteric, gastroduodenal, hepatic and renal arteries are some of the common arteries affected by VAAs. Though surgical resection and anastomosis still remains the treatment of choice in some of the cases, especially cases involving the proximal arteries, increasingly endovascular treatment is being used for more distal vessels. We present a pictorial review of various intra-abdominal VAAs and their endovascular management.
Keywords: Coil embolization; Endovascular management; Imaging; Pseudoaneurysm; Visceral arterial aneurysm.
Figures

References
-
- Shanley CJ, Shah NL, Messina LM. Common splanchnic artery aneurysms: splenic, hepatic, and celiac. Ann Vasc Surg. 1996;10:315–322. - PubMed
-
- Liu Q, Lu JP, Wang F, Wang L, Jin AG, Wang J, Tian JM. Visceral artery aneurysms: evaluation using 3D contrast-enhanced MR angiography. AJR Am J Roentgenol. 2008;191:826–833. - PubMed
-
- Hallett JW. Splenic artery aneurysms. Semin Vasc Surg. 1995;8:321–326. - PubMed
-
- Gabelmann A, Görich J, Merkle EM. Endovascular treatment of visceral artery aneurysms. J Endovasc Ther. 2002;9:38–47. - PubMed
-
- O'Driscoll D, Olliff SP, Olliff JF. Hepatic artery aneurysm. Br J Radiol. 1999;72:1018–1025. - PubMed
LinkOut - more resources
Full Text Sources
