

A randomized, phase III trial of capecitabine plus bevacizumab (Cape-Bev) versus capecitabine plus irinotecan plus bevacizumab (CAPIRI-Bev) in first-line treatment of metastatic colorectal cancer: the AIO KRK 0110 trial/ML22011 trial
- PMID: 21861888
- PMCID: PMC3173448
- DOI: 10.1186/1471-2407-11-367
A randomized, phase III trial of capecitabine plus bevacizumab (Cape-Bev) versus capecitabine plus irinotecan plus bevacizumab (CAPIRI-Bev) in first-line treatment of metastatic colorectal cancer: the AIO KRK 0110 trial/ML22011 trial
Abstract
Background: Several randomized trials have indicated that combination chemotherapy applied in metastatic colorectal cancer (mCRC) does not significantly improve overall survival when compared to the sequential use of cytotoxic agents (CAIRO, MRC Focus, FFCD 2000-05). The present study investigates the question whether this statement holds true also for bevacizumab-based first-line treatment including escalation- and de-escalation strategies.
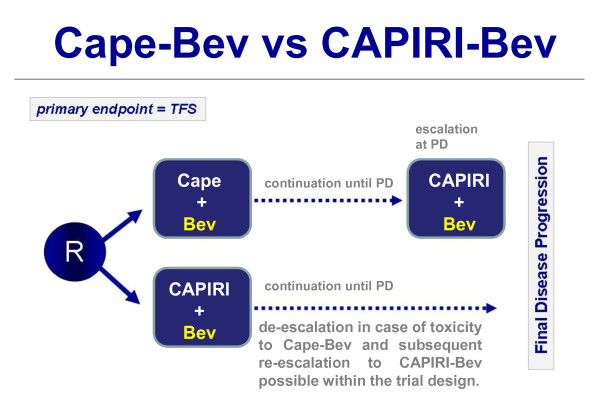
Methods/design: The AIO KRK 0110/ML22011 trial is a two-arm, multicenter, open-label randomized phase III trial comparing the efficacy and safety of capecitabine plus bevacizumab (Cape-Bev) versus capecitabine plus irinotecan plus bevacizumab (CAPIRI-Bev) in the first-line treatment of metastatic colorectal cancer. Patients with unresectable metastatic colorectal cancer, Eastern Cooperative Oncology Group (ECOG) performance status 0-1, will be assigned in a 1:1 ratio to receive either capecitabine 1250 mg/m(2) bid for 14d (d1-14) plus bevacizumab 7.5 mg/kg (d1) q3w (Arm A) or capecitabine 800 mg/m(2) BID for 14d (d1-14), irinotecan 200 mg/m(2) (d1) and bevacizumab 7.5 mg/kg (d1) q3w (Arm B). Patients included into this trial are required to consent to the analysis of tumour tissue and blood for translational investigations. In Arm A, treatment escalation from Cape-Bev to CAPIRI-Bev is recommended in case of progressive disease (PD). In Arm B, de-escalation from CAPIRI-Bev to Cape-Bev is possible after 6 months of treatment or in case of irinotecan-associated toxicity. Re-escalation to CAPIRI-Bev after PD is possible. The primary endpoint is time to failure of strategy (TFS). Secondary endpoints are overall response rate (ORR), overall survival, progression-free survival, safety and quality of life.
Conclusion: The AIO KRK 0110 trial is designed for patients with disseminated, but asymptomatic mCRC who are not potential candidates for surgical resection of metastasis. Two bevacizumab-based strategies are compared: one starting as single-agent chemotherapy (Cape-Bev) allowing escalation to CAPIRI-Bev and another starting with combination chemotherapy (CAPIRI-Bev) and allowing de-escalation to Cape-Bev and subsequent re-escalation if necessary.
Trial registration: ClinicalTrials.gov Identifier NCT01249638 EudraCT-No.: 2009-013099-38.
Figures
References
-
- Adam R, Haller DG, Poston G, Raoul J-L, Spano J-P, Tabernero J, Van Cutsem E. Toward optimized front-line therapeutic strategies in patients with metastatic colorectal cancer--an expert review from the International Congress on Anti-Cancer Treatment (ICACT) 2009. Annals of Oncology. 2010. - PubMed
-
- Petrelli NJ, Abbruzzese J, Mansfield P, Minsky B. Hepatic resection: the last surgical frontier for colorectal cancer. J Clin Oncol. 2005;23(20):4475–7. - PubMed
-
- Feliu J, Salut A, Safont M, Losa F, Garcia C, Bosch C, Escudero P, Lopez R, Bolanos M, Gonzalez-Baron M. ONCOPAZ group. First-line treatment with bevacizumab plus capecitabine for elderly patients with metastatic colorectal cancer: BECA trial. ASCO Meeting Abstracts. 2008;26(15_suppl):15120.
-
- Tebbutt NC, Wilson K, Gebski VJ, Cummins MM, Zannino D, van Hazel GA, Robinson B, Broad A, Ganju V, Ackland SP, Forgeson G, Cunningham D, Saunders MP, Stockler MR, Chua Y, Zalcberg JR, Simes RJ, Price TJ. Capecitabine, bevacizumab, and mitomycin in first-line treatment of metastatic colorectal cancer: results of the Australasian Gastrointestinal Trials Group Randomized Phase III MAX Study. J Clin Oncol. 2010;28(19):3191–8. doi: 10.1200/JCO.2009.27.7723. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
