

Immunological applications of stem cells in type 1 diabetes
- PMID: 21862682
- PMCID: PMC3591677
- DOI: 10.1210/er.2011-0008
Immunological applications of stem cells in type 1 diabetes
Abstract
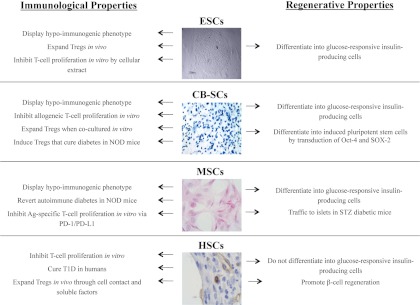
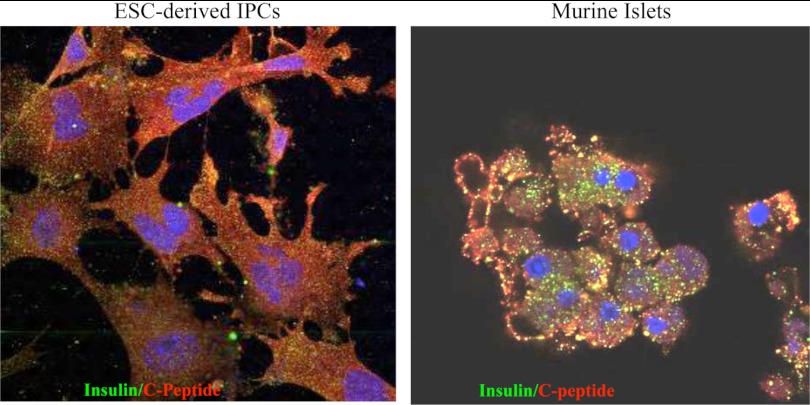
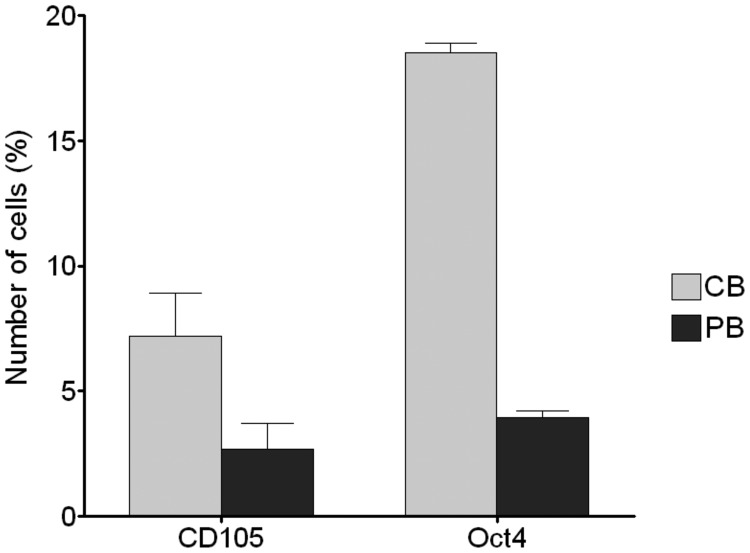
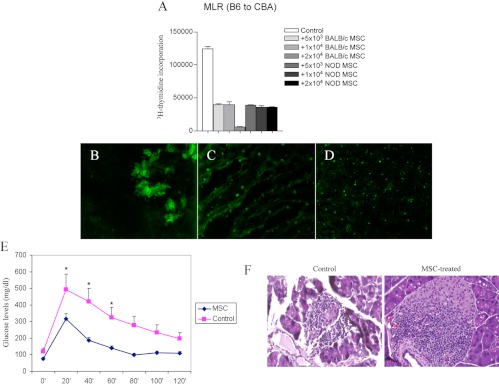
Current approaches aiming to cure type 1 diabetes (T1D) have made a negligible number of patients insulin-independent. In this review, we revisit the role of stem cell (SC)-based applications in curing T1D. The optimal therapeutic approach for T1D should ideally preserve the remaining β-cells, restore β-cell function, and protect the replaced insulin-producing cells from autoimmunity. SCs possess immunological and regenerative properties that could be harnessed to improve the treatment of T1D; indeed, SCs may reestablish peripheral tolerance toward β-cells through reshaping of the immune response and inhibition of autoreactive T-cell function. Furthermore, SC-derived insulin-producing cells are capable of engrafting and reversing hyperglycemia in mice. Bone marrow mesenchymal SCs display a hypoimmunogenic phenotype as well as a broad range of immunomodulatory capabilities, they have been shown to cure newly diabetic nonobese diabetic (NOD) mice, and they are currently undergoing evaluation in two clinical trials. Cord blood SCs have been shown to facilitate the generation of regulatory T cells, thereby reverting hyperglycemia in NOD mice. T1D patients treated with cord blood SCs also did not show any adverse reaction in the absence of major effects on glycometabolic control. Although hematopoietic SCs rarely revert hyperglycemia in NOD mice, they exhibit profound immunomodulatory properties in humans; newly hyperglycemic T1D patients have been successfully reverted to normoglycemia with autologous nonmyeloablative hematopoietic SC transplantation. Finally, embryonic SCs also offer exciting prospects because they are able to generate glucose-responsive insulin-producing cells. Easy enthusiasm should be mitigated mainly because of the potential oncogenicity of SCs.
Copyright © 2011 by The Endocrine Society
Figures
References
-
- Colucci F, Cilio CM. 2010. Taming killer cells may halt diabetes progression. Nat Immunol 11:111–112 - PubMed
-
- Patterson CC, Dahlquist GG, Gyürüs E, Green A, Soltész G. 2009. Incidence trends for childhood type 1 diabetes in Europe during 1989–2003 and predicted new cases 2005–20: a multicentre prospective registration study. Lancet 373:2027–2033 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
