

Progression of left ventricular diastolic dysfunction and risk of heart failure
- PMID: 21862747
- PMCID: PMC3269764
- DOI: 10.1001/jama.2011.1201
Progression of left ventricular diastolic dysfunction and risk of heart failure
Abstract
Context: Heart failure incidence increases with advancing age, and approximately half of patients with heart failure have preserved left ventricular ejection fraction. Although diastolic dysfunction plays a role in heart failure with preserved ejection fraction, little is known about age-dependent longitudinal changes in diastolic function in community populations.
Objective: To measure changes in diastolic function over time and to determine the relationship between diastolic dysfunction and the risk of subsequent heart failure.
Design, setting, and participants: Population-based cohort of participants enrolled in the Olmsted County Heart Function Study. Randomly selected participants 45 years or older (N = 2042) underwent clinical evaluation, medical record abstraction, and echocardiography (examination 1 [1997-2000]). Diastolic left ventricular function was graded as normal, mild, moderate, or severe by validated Doppler techniques. After 4 years, participants were invited to return for examination 2 (2001-2004). The cohort of participants returning for examination 2 (n = 1402 of 1960 surviving [72%]) then underwent follow-up for ascertainment of new-onset heart failure (2004-2010).
Main outcome measures: Change in diastolic function grade and incident heart failure.
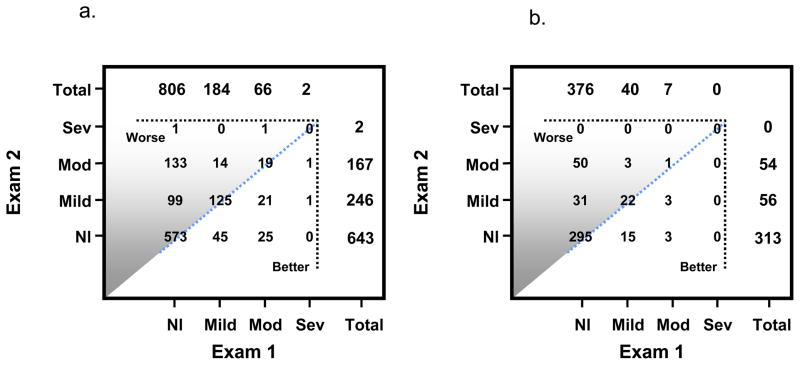
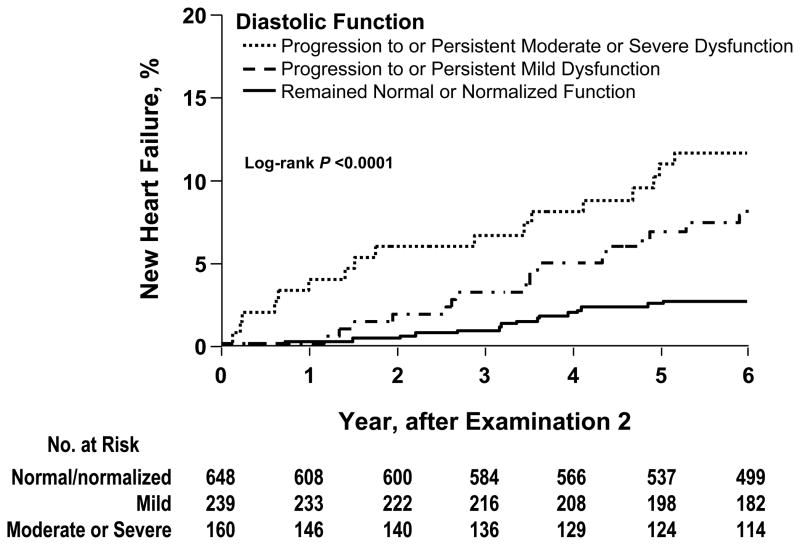
Results: During the 4 (SD, 0.3) years between examinations 1 and 2, diastolic dysfunction prevalence increased from 23.8% (95% confidence interval [CI], 21.2%-26.4%) to 39.2% (95% CI, 36.3%-42.2%) (P < .001). Diastolic function grade worsened in 23.4% (95% CI, 20.9%-26.0%) of participants, was unchanged in 67.8% (95% CI, 64.8%-70.6%), and improved in 8.8% (95% CI, 7.1%-10.5%). Worsened diastolic dysfunction was associated with age 65 years or older (odds ratio, 2.85 [95% CI, 1.77-4.72]). During 6.3 (SD, 2.3) years of additional follow-up, heart failure occurred in 2.6% (95% CI, 1.4%-3.8%), 7.8% (95% CI, 5.8%-13.0%), and 12.2% (95% CI, 8.5%-18.4%) of persons whose diastolic function normalized or remained normal, remained or progressed to mild dysfunction, or remained or progressed to moderate or severe dysfunction, respectively (P < .001). Diastolic dysfunction was associated with incident heart failure after adjustment for age, hypertension, diabetes, and coronary artery disease (hazard ratio, 1.81 [95% CI, 1.01-3.48]).
Conclusions: In a population-based cohort undergoing 4 years of follow-up, prevalence of diastolic dysfunction increased. Diastolic dysfunction was associated with development of heart failure during 6 years of subsequent follow-up.
Conflict of interest statement
Conflict of Interest Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Intersst.
Figures
References
-
- Rodeheffer RJ, Jacobsen SJ, Gersh BJ, et al. The incidence and prevalence of congestive heart failure in Rochester, Minnesota. Mayo Clin Proc. 1993;68:1143–1150. - PubMed
-
- McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med. 1971;285:1441–1446. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–1402. - PubMed
-
- Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the community: trends in incidence and survival in a 10-year period. Arch Intern Med. 1999;159:29–34. - PubMed
-
- Mosterd A, Hoes AW, de Bruyne MC, et al. Prevalence of heart failure and left ventricular dysfunction in the general population; The Rotterdam Study. Eur Heart J. 1999;20:447–455. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
