

Association of bronchopulmonary dysplasia and hypercarbia in ventilated infants with birth weights of 500-1,499 g
- PMID: 21863239
- PMCID: PMC3397775
- DOI: 10.1007/s10995-011-0863-0
Association of bronchopulmonary dysplasia and hypercarbia in ventilated infants with birth weights of 500-1,499 g
Abstract
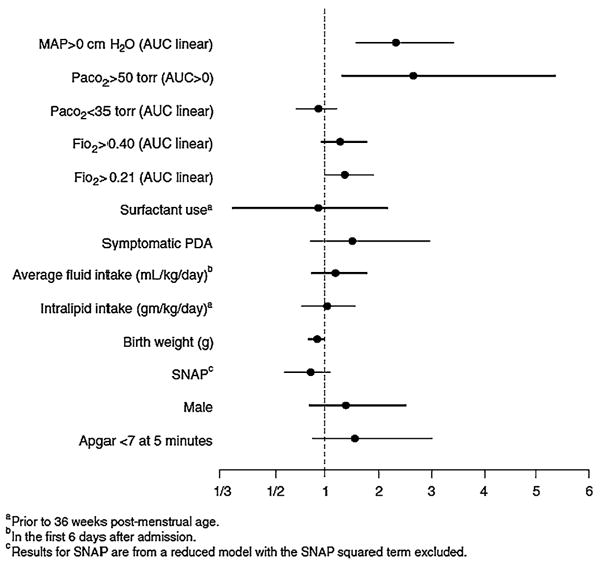
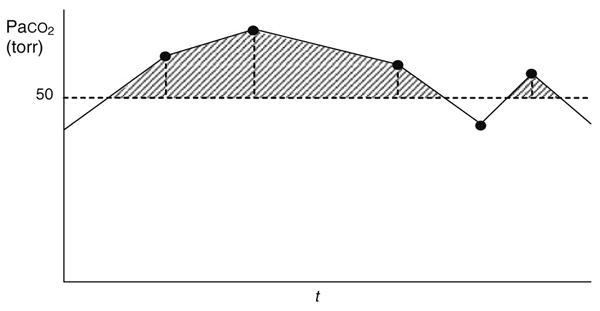
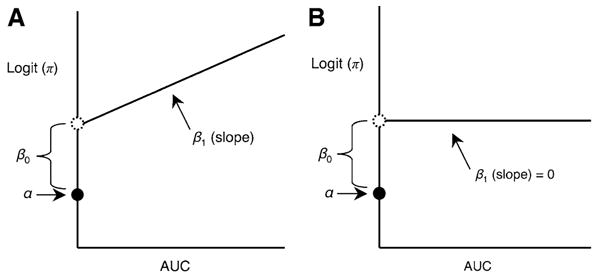
Bronchopulmonary dysplasia (BPD) continues to be a major pulmonary complication in very low birth weight (VLBW) and extremely low birth weight (ELBW) survivors of neonatal intensive care units (NICUs). Many factors including partial pressures of carbon dioxide (PaCO: (2)) have been implicated as possible causes. Permissive hypercapnia has become a more common practice in ventilated infants, but its effect on BPD is unclear. The hypothesis of this study was that hypercarbia is associated with increased BPD in infants with birth weights of 500-1,499 g. Nine hospitals were involved in this observational cohort study. Maternal and infant information including socio-demographics, antenatal steroids, gender, race, gestational age, birth weight, intubation and ventilator status, physiologic variables and data on therapies were collected by chart abstraction. SNAP scores were assigned. Candidate BPD risk factors, including cumulative exposures derived from blood gas and ventilation data in the first 6 days of life, were identified. Risk models were developed for 425 preterm infants who survived to 36 weeks post-menstrual age. BPD occurrence was associated with the cumulative burden of MAP >0 cm H(2)O in the first 6 days of life (P < 0.0001). After adjustment for the burden of MAP, the occurrence of hypercarbia (PaCO: (2) >50 torr) was associated with a greater incidence of BPD (P = 0.024). Among 293 intubated, mechanically ventilated infants, those with hypercarbia occurring only when MAP ≤ 8 cm H(2)O, a scenario more comparable to permissive hypercapnia, also had increased BPD incidence compared to infants without hypercarbia (P = 0.0003). Hypercarbia during the first 6 days of life was associated with increased incidence of BPD in these infants. Mechanically ventilated infants with hypercarbia during low MAP also had a significant increase in BPD. Permissive hypercapnia in ventilated infants needs further close review before the practice becomes even more widespread.
Figures
References
-
- Northway WH., Jr Bronchopulmonary dysplasia thirty three years later. Pediatric Pulmonology. 2001;26(S23):5–7. - PubMed
-
- Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB, Papile LA, et al. Very low birth weight outcomes of the NICHD Neonatal Research Network, January 1993 to December 1994. American Journal of Obstetrics and Gynecology. 1998;179(6):1632–1639. - PubMed
-
- Wung JT, James LS, Kilchevsky E, James E. Management of infants with severe respiratory failure and persistence of the fetal circulation, without hyperventilation. Pediatrics. 1985;76(4):488–494. - PubMed
-
- Hickling KG, Walsh J, Henderson S, Jackson R. Low mortality rate in adult respiratory distress syndrome using low-volume, pressure-limited ventilation with permissive hypercapnia: A prospective study. Critical Care Medicine. 1994;22(10):1568–1578. - PubMed
Publication types
MeSH terms
Grants and funding
- U18-HD30445/HD/NICHD NIH HHS/United States
- U18 HD030445/HD/NICHD NIH HHS/United States
- U18 HD030447/HD/NICHD NIH HHS/United States
- U18-HD30454/HD/NICHD NIH HHS/United States
- U10 HD030445/HD/NICHD NIH HHS/United States
- U18-HD30447/HD/NICHD NIH HHS/United States
- U18-HD30458/HD/NICHD NIH HHS/United States
- U18 HD031919/HD/NICHD NIH HHS/United States
- U18-HD30450/HD/NICHD NIH HHS/United States
- U18-HD31919/HD/NICHD NIH HHS/United States
- U10 HD047890/HD/NICHD NIH HHS/United States
- U18-HD31206/HD/NICHD NIH HHS/United States
- U18 HD031206/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
