

Aurora kinase inhibition overcomes cetuximab resistance in squamous cell cancer of the head and neck
- PMID: 21865609
- PMCID: PMC3248211
- DOI: 10.18632/oncotarget.311
Aurora kinase inhibition overcomes cetuximab resistance in squamous cell cancer of the head and neck
Abstract
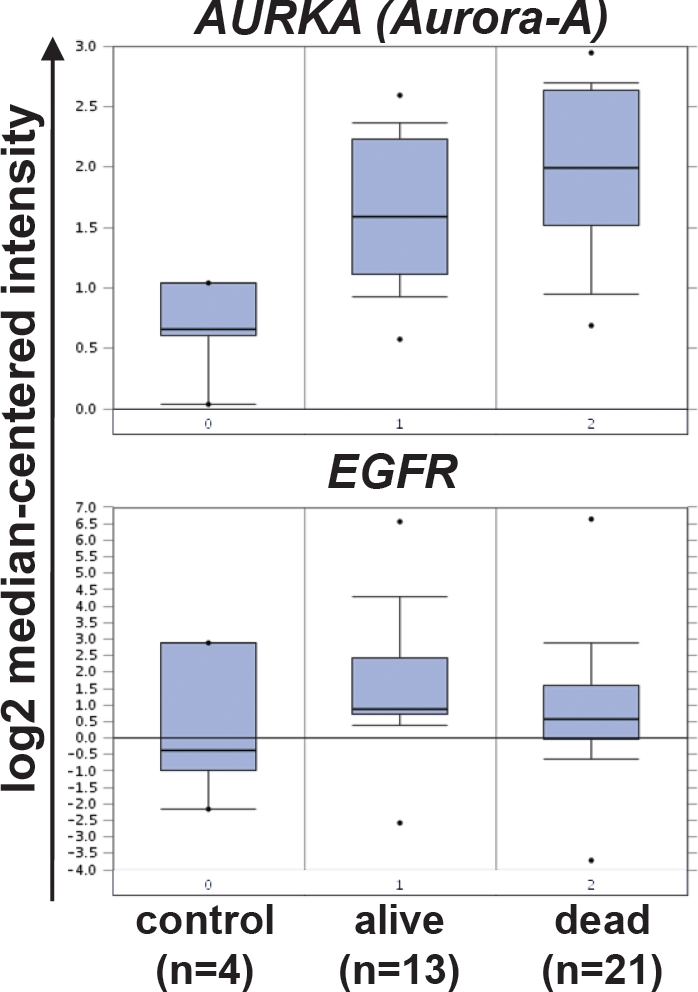
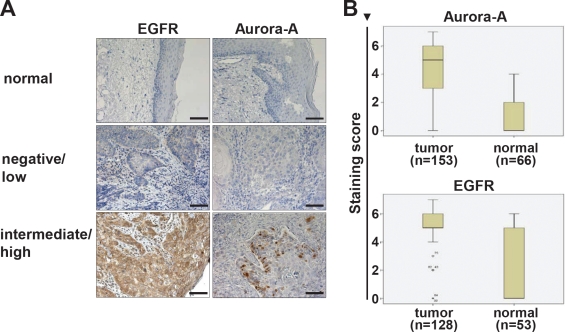
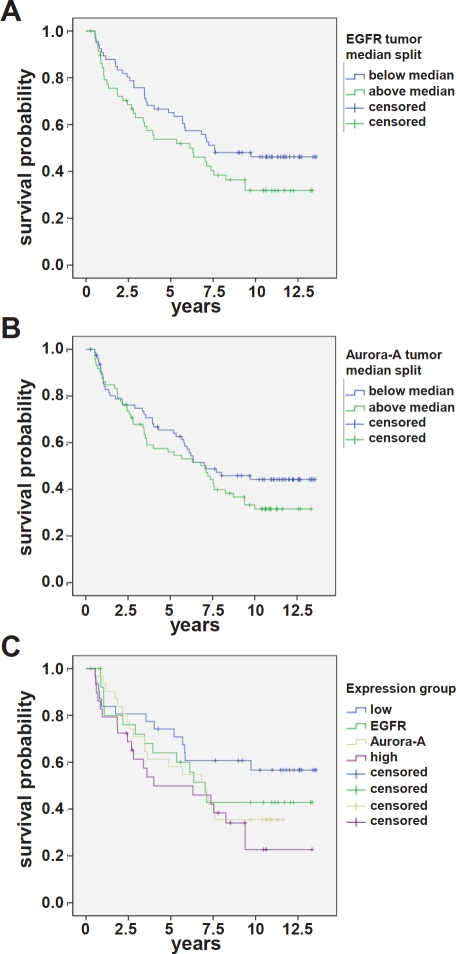
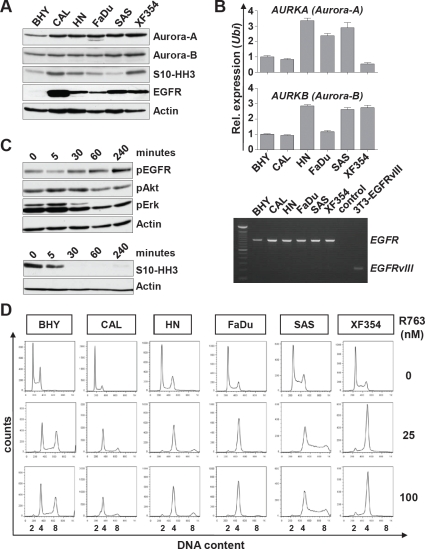
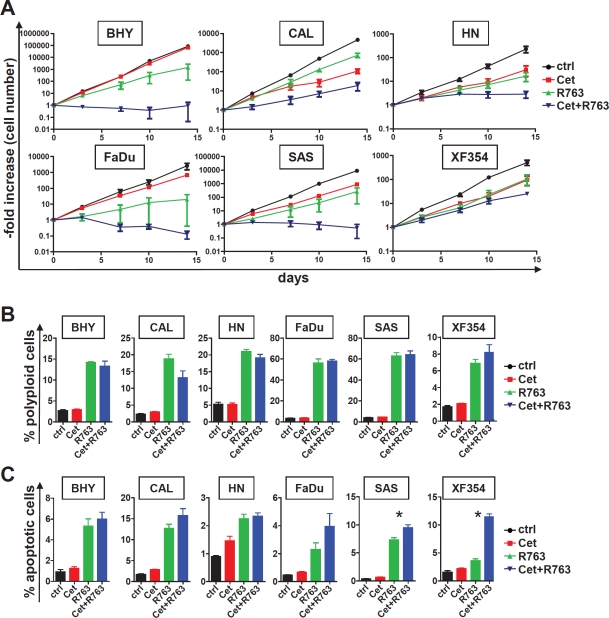
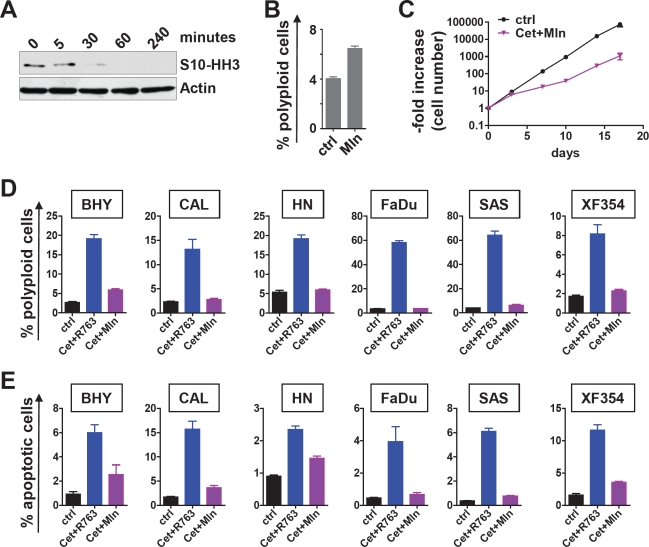
Squamous cell cancer of the head and neck (SCCHN) is the sixth leading cause for cancer deaths worldwide. Despite extense knowledge of risk factors and pathogenesis about 50 percent of all patients and essentially every patient with metastatic SCCHN eventually die from this disease. We analyzed the clinical data and performed immunohistochemistry for Epidermal growth factor receptor (EGFR) and Aurora kinase A (Aurora-A) expression in 180 SCCHN patients. Patients characterized by elevated EGFR and elevated Aurora-A protein expression in tumor tissue represent a risk group with poor disease-free and overall survival (EGFR(low)Aurora-A(low) versus EGFR(high)Aurora-A(high), p = 0.024). Treating SCCHN cell lines with a pan-Aurora kinase inhibitor resulted in defective cytokinesis, polyploidy and apoptosis, which was effective irrespective of the EGFR status. Combined Aurora kinase and EGFR targeting using a monoclonal anti-EGFR antibody was more effective compared to single EGFR and Aurora kinase inhibition. Comparing pan-Aurora kinase and Aurora-A targeting hints towards a strong and clinically relevant biological effect mediated via Aurora kinase B. Taken together, our findings characterize a new poor risk group in SCCHN patients defined by elevated EGFR and Aurora-A protein expression. Our results demonstrate that combined targeting of EGFR and Aurora kinases represents a therapeutic means to activate cell cycle checkpoints and apoptosis in SCCHN.
Conflict of interest statement
The authors declare no potential conflicts of interests.
Figures
Similar articles
-
Epidermal Growth Factor Receptor Inhibition in Squamous Cell Carcinoma of the Head and Neck.Hematol Oncol Clin North Am. 2015 Dec;29(6):1011-32. doi: 10.1016/j.hoc.2015.07.007. Hematol Oncol Clin North Am. 2015. PMID: 26568545 Review.
-
Inhibition of TGF-β enhances the in vivo antitumor efficacy of EGF receptor-targeted therapy.Mol Cancer Ther. 2012 Nov;11(11):2429-39. doi: 10.1158/1535-7163.MCT-12-0101-T. Epub 2012 Aug 27. Mol Cancer Ther. 2012. PMID: 22927667 Free PMC article.
-
Preclinical modeling of EGFR inhibitor resistance in head and neck cancer.Cancer Biol Ther. 2012 Aug;13(10):935-45. doi: 10.4161/cbt.20846. Epub 2012 Aug 1. Cancer Biol Ther. 2012. PMID: 22785204 Free PMC article.
-
Establishment and characterization of a model of acquired resistance to epidermal growth factor receptor targeting agents in human cancer cells.Clin Cancer Res. 2009 Mar 1;15(5):1585-92. doi: 10.1158/1078-0432.CCR-08-2068. Epub 2009 Feb 3. Clin Cancer Res. 2009. PMID: 19190133 Free PMC article.
-
New approaches to EGFR inhibition for locally advanced or metastatic squamous cell carcinoma of the head and neck (SCCHN).Med Oncol. 2012 Dec;29(4):2481-91. doi: 10.1007/s12032-012-0159-2. Epub 2012 Jan 18. Med Oncol. 2012. PMID: 22252310 Free PMC article. Review.
Cited by
-
Potential impact of human papilloma virus on survival of basaloid squamous carcinoma of the head and neck.Oncotarget. 2015 Feb 20;6(5):3462-70. doi: 10.18632/oncotarget.3062. Oncotarget. 2015. PMID: 25739121 Free PMC article.
-
Scientific Rationale Supporting the Clinical Development Strategy for the Investigational Aurora A Kinase Inhibitor Alisertib in Cancer.Front Oncol. 2015 Aug 24;5:189. doi: 10.3389/fonc.2015.00189. eCollection 2015. Front Oncol. 2015. PMID: 26380220 Free PMC article. Review.
-
Dual Aurora A and JAK2 kinase blockade effectively suppresses malignant transformation.Oncotarget. 2014 May 30;5(10):2947-61. doi: 10.18632/oncotarget.1615. Oncotarget. 2014. PMID: 24930769 Free PMC article.
-
Selective Targeting of CTNBB1-, KRAS- or MYC-Driven Cell Growth by Combinations of Existing Drugs.PLoS One. 2015 May 27;10(5):e0125021. doi: 10.1371/journal.pone.0125021. eCollection 2015. PLoS One. 2015. PMID: 26018524 Free PMC article.
-
Mechanisms of resistance in head and neck cancer.Am J Cancer Res. 2020 Sep 1;10(9):2742-2751. eCollection 2020. Am J Cancer Res. 2020. PMID: 33042614 Free PMC article. Review.
References
-
- Hunter KD, Parkinson EK, Harrison PR. Profiling early head and neck cancer. Nat Rev Cancer. 2005;5:127–135. - PubMed
-
- Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, Erfan J, Zabolotnyy D, Kienzer HR, Cupissol D, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359:1116–1127. - PubMed
-
- Forastiere A, Koch W, Trotti A, Sidransky D. Head and neck cancer. N Engl J Med. 2001;345:1890–1900. - PubMed
-
- Haddad RI, Shin DM. Recent advances in head and neck cancer. N Engl J Med. 2008;359:1143–1154. - PubMed
-
- Jin C, Jin Y, Wennerberg J, Akervall J, Dictor M, Mertens F. Karyotypic heterogeneity and clonal evolution in squamous cell carcinomas of the head and neck. Cancer Genet Cytogenet. 2002;132:85–96. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
