

Is surgical resection superior to transplantation in the treatment of hepatocellular carcinoma?
- PMID: 21865950
- PMCID: PMC4425302
- DOI: 10.1097/SLA.0b013e31822ca66f
Is surgical resection superior to transplantation in the treatment of hepatocellular carcinoma?
Abstract
Objective: To compare outcomes for patients with hepatocellular carcinoma (HCC) treated with either liver resection or transplantation.
Methods: A retrospective, single-institution analysis of 413 HCC patients from 1999 to 2009.
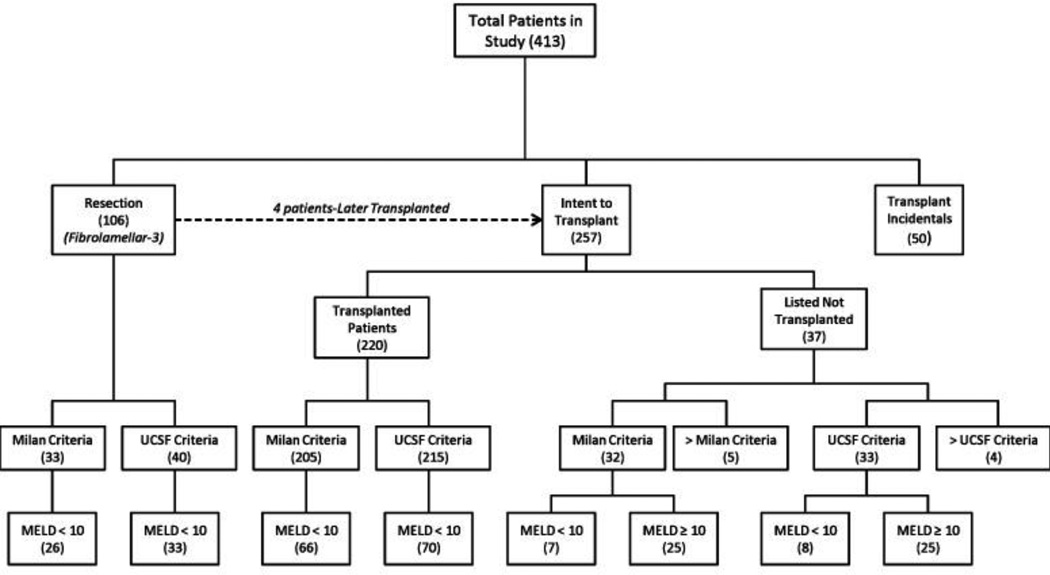
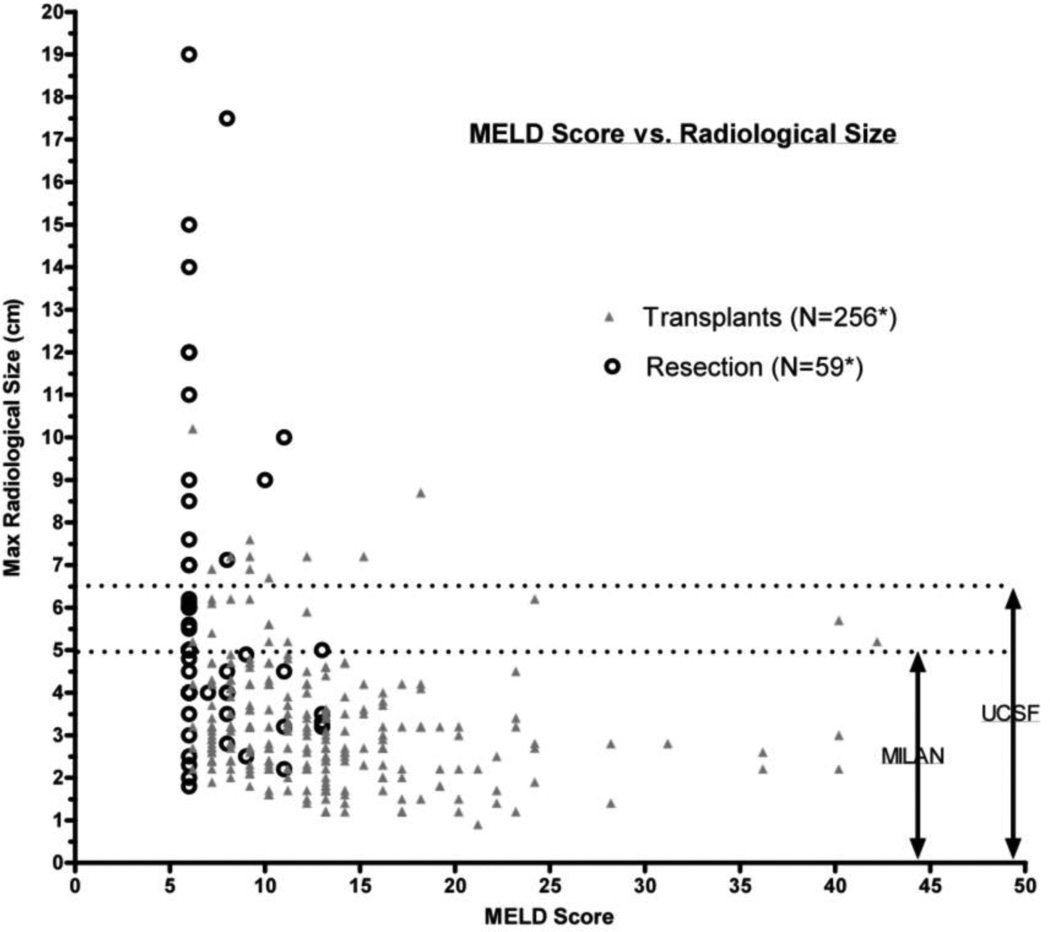
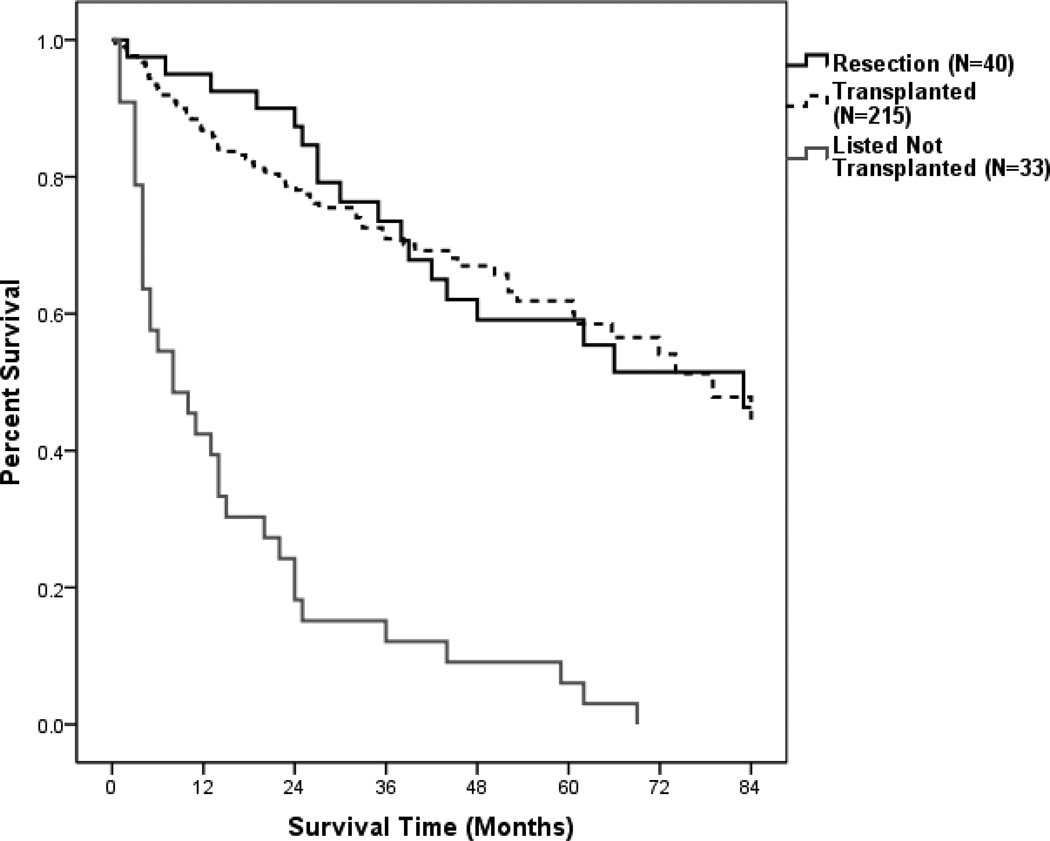
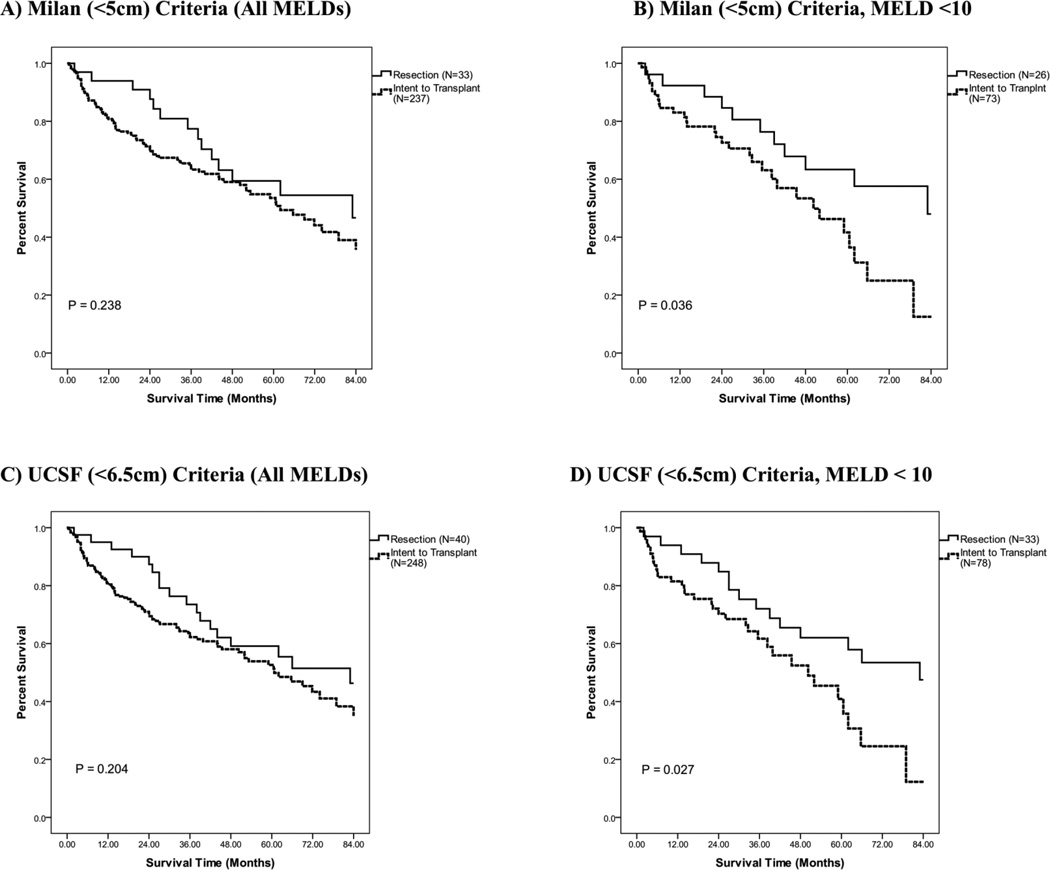
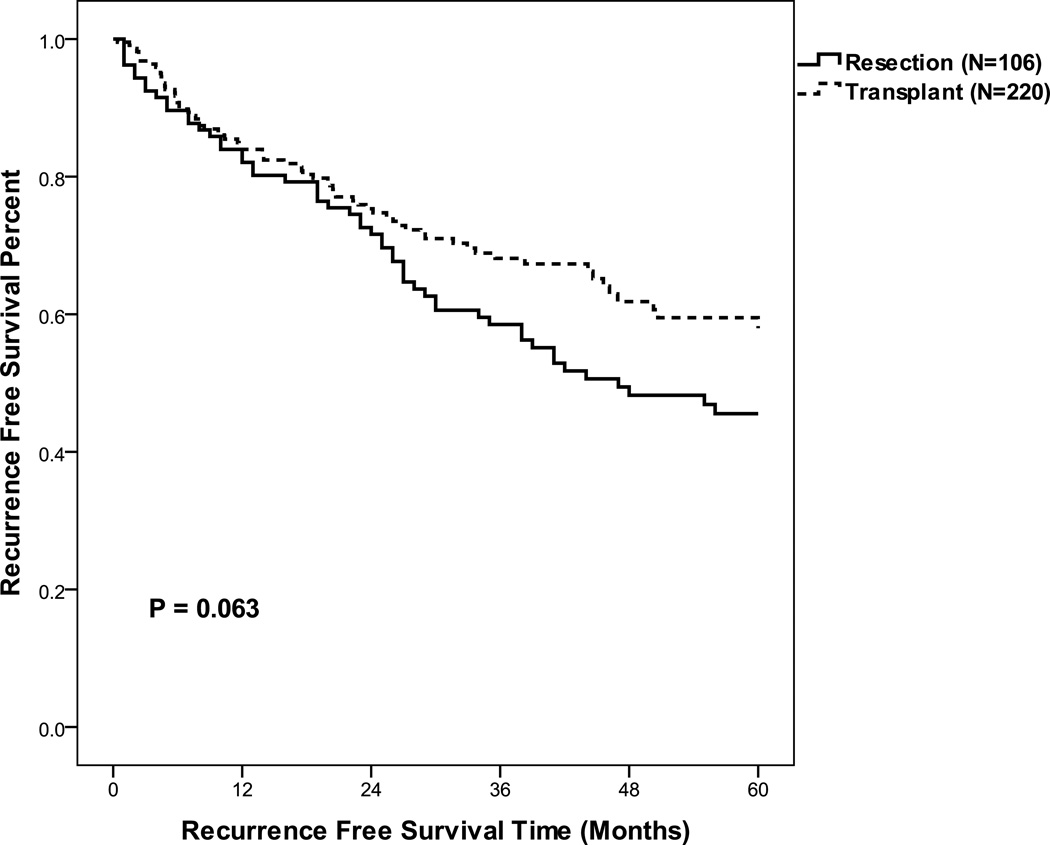
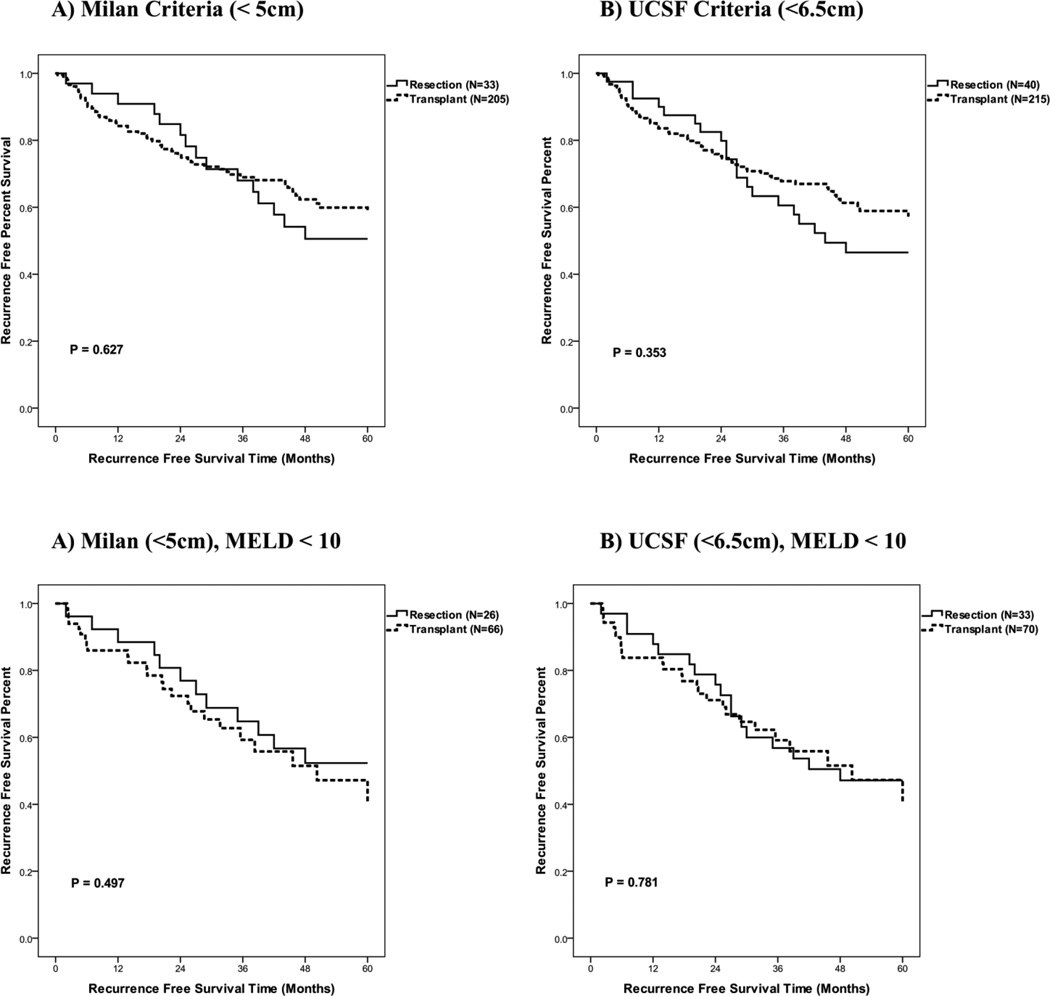
Results: A total of 413 patients with HCC underwent surgical resection (n = 106) and transplantation (n = 270) or were listed without receiving transplantation (n = 37). Excluding transplanted patients with incidental tumors (n = 50), 257 patients with suspected HCC were listed with the intent to transplant (ITT). The median diameter of the largest tumor by radiography was 6.0 cm in resected, 3.0 cm in transplanted, and 3.4 cm in the listed-but-not-transplanted patients. Median time to transplant was 48 days. Recurrence rates were 19.8% for resection and 12.1% for all ITT patients. Overall, patient survival for resection versus ITT patients was similar (5-year survival of 53.0% vs 52.0%, not significant). However, for HCC patients with model end-stage liver disease (MELD) scores less than 10 and who radiologically met Milan or UCSF (University of California, San Francisco) criteria, 1-year and 5-year survival rates were significantly improved in resected patients. For patients with MELD score less than 10 and who met Milan criteria, 1-year and 5-year survival were 92.0% and 63.0% for resection (n = 26) versus 83.0% and 41.0% for ITT (n = 73, P = 0.036). For those with MELD score less than 10 and met UCSF criteria, 1-year and 5-year survival was 94.0% and 62.0% for resection (n = 33) versus 81.0% and 40.0% for ITT (n = 78, P = 0.027).
Conclusions: Among known HCC patients with preserved liver function, resection was associated with superior patient survival versus transplantation. These results suggest that surgical resection should remain the first line therapy for patients with HCC and compensated liver function who are candidates for resection.
Figures
References
-
- World Health Organization. [Accessed May 1, 2011]; Website: http://www.who.int/mediacentre/factsheets/fs297/en/index.html.
-
- El-Serag HB. Hepatocellular carcinoma: recent trends in the United States. Gastroenterology. 2004;127(5) Suppl 1:S27–S34. - PubMed
-
- Bosch FX, Ribes J, Diaz M, Cleries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127(5) Suppl 1:S5–S16. - PubMed
-
- Bruno S, Silini E, Crosignani A, Borzio F, Leandro G, Bono F, et al. Hepatitis C virus genotypes and risk of hepatocellular carcinoma in cirrhosis: a prospective study. Hepatology. 1997;25(3):754–758. - PubMed
-
- McKillop IH, Moran DM, Jin X, Koniaris LG. Molecular pathogenesis of hepatocellular carcinoma. J Surg Res. 2006;136(1):125–135. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
