

Single-incision vaginal approach to treat cystocele and vault prolapse with an anterior wall mesh anchored apically to the sacrospinous ligaments
- PMID: 21866442
- PMCID: PMC3251774
- DOI: 10.1007/s00192-011-1536-7
Single-incision vaginal approach to treat cystocele and vault prolapse with an anterior wall mesh anchored apically to the sacrospinous ligaments
Abstract
Introduction and hypothesis: The safety and early efficacy of a new technique to treat cystocele and/or concomitant apical prolapse through a single vaginal incision with a lightweight mesh anchored apically bilaterally to the sacrospinous ligaments is reported.
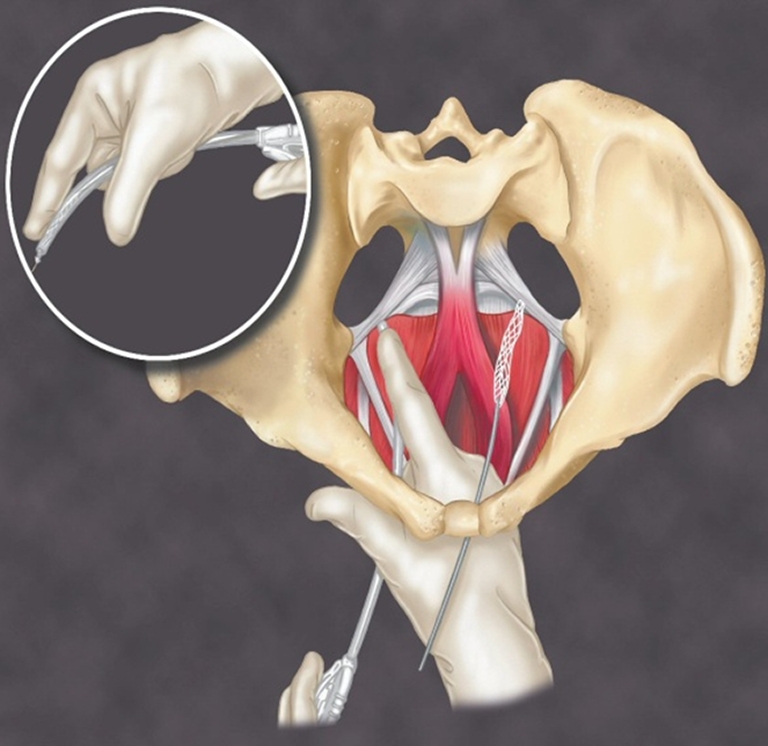
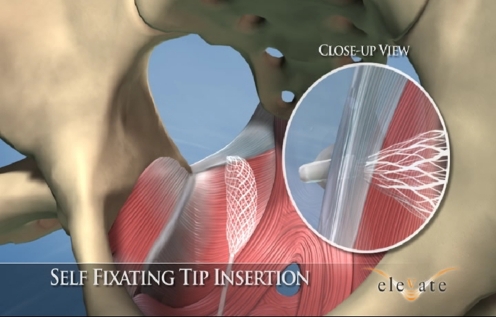
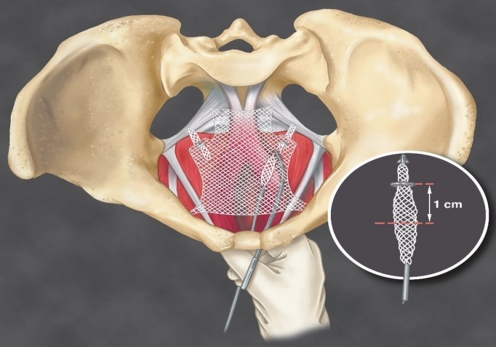
Methods: Women with anterior compartment and/or apical prolapse ≥ stage II underwent repair through a single anterior vaginal wall incision with the Anterior Elevate System (AES). The technique utilizes a lightweight (24 g/m(2)) type I mesh anchored to the sacrospinous ligaments via two mesh arms with small self-fixating tips. The bladder neck portion of the graft is anchored to the obturator internus with similar self-fixating tips. The apical portion of the graft is adjustable to vaginal length prior to locking in place. Outcome measures included prolapse degree at last follow-up visit, intra/post-operative complications, and QOL assessments.
Results: Sixty patients were implanted with average follow-up of 13.4 months (range 3-24 months). Mean pre-op Ba was +2.04 ± 1.3 and C -2.7 ± 2.9. Average blood loss was 47 cc and average hospital stay was 23 h. Sixty-two percent of patients had concomitant sling for SUI. Mean post-op Ba is -2.45 ± 0.9 and C -8.3 ± 0.9. There was no statistical difference in pre- to post-op TVL. Objective cure rate at current follow-up is 91.7% (≤ stage 1). To date, there have been no mesh extrusions. No patients have reported significant buttock or leg pain. No patients have required surgical revision for any reason.
Conclusion: The AES is a minimally invasive technique to treat anterior compartment and/or apical prolapse through a single vaginal incision. Initial results show the procedure to be safe and early efficacy is promising. Longer-term follow-up is ongoing.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
