

C-reactive protein and prediction of 1-year mortality in prevalent hemodialysis patients
- PMID: 21868617
- PMCID: PMC3186454
- DOI: 10.2215/CJN.00710111
C-reactive protein and prediction of 1-year mortality in prevalent hemodialysis patients
Abstract
Background and objectives: Measurement of C-reactive protein (CRP) levels remains uncommon in North America, although it is now routine in many countries. Using Dialysis Outcomes and Practice Patterns Study data, our primary aim was to evaluate the value of CRP for predicting mortality when measured along with other common inflammatory biomarkers.
Design, setting, participants, & measurements: We studied 5061 prevalent hemodialysis patients from 2005 to 2008 in 140 facilities routinely measuring CRP in 10 countries. The association of CRP with mortality was evaluated using Cox regression. Prediction of 1-year mortality was assessed in logistic regression models with differing adjustment variables.
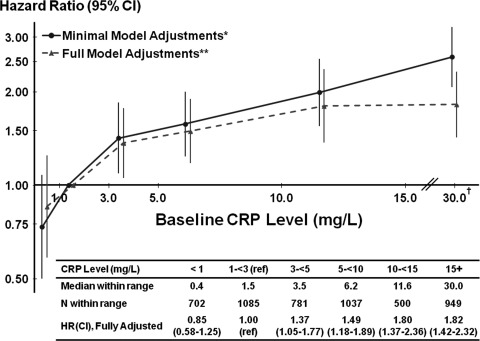
Results: Median baseline CRP was lower in Japan (1.0 mg/L) than other countries (6.0 mg/L). CRP was positively, monotonically associated with mortality. No threshold below which mortality rate leveled off was identified. In prediction models, CRP performance was comparable with albumin and exceeded ferritin and white blood cell (WBC) count based on measures of model discrimination (c-statistics, net reclassification improvement [NRI]) and global model fit (generalized R(2)). The primary analysis included age, gender, diabetes, catheter use, and the four inflammatory markers (omitting one at a time). Specifying NRI ≥5% as appropriate reclassification of predicted mortality risk, NRI for CRP was 12.8% compared with 10.3% for albumin, 0.8% for ferritin, and <0.1% for WBC.
Conclusions: These findings demonstrate the value of measuring CRP in addition to standard inflammatory biomarkers to improve mortality prediction in hemodialysis patients. Future studies are indicated to identify interventions that lower CRP and to identify whether they improve clinical outcomes.
Figures




References
-
- U.S. Renal Data System: USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2010
-
- Owen WF, Lowrie EG: C-reactive protein as an outcome predictor for maintenance hemodialysis patients. Kidney Int 54: 627–636, 1998 - PubMed
-
- Yeun JY, Levine RA, Mantadilok V, Kaysen GA: C-reactive protein predicts all-cause and cardiovascular mortality in hemodialysis patients. Am J Kidney Dis 35: 469–476, 2000 - PubMed
-
- Zimmermann J, Herrlinger S, Pruy A, Metzger T, Wanner C: Inflammation enhances cardiovascular risk and mortality in hemodialysis patients. Kidney Int 55: 648–658, 1999 - PubMed
-
- deFilippi C, Wasserman S, Rosanio S, Tiblier E, Sperger H, Tocchi M, Christenson R, Uretsky B, Smiley M, Gold J, Muniz H, Badalamenti J, Herzog C, Henrich W: Cardiac troponin T and C-reactive protein for predicting prognosis, coronary atherosclerosis, and cardiomyopathy in patients undergoing long-term hemodialysis. J Am Med Assoc 290: 353–359, 2003 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
