

Regulatory T cells limit vascular endothelial injury and prevent pulmonary hypertension
- PMID: 21868697
- PMCID: PMC3204361
- DOI: 10.1161/CIRCRESAHA.110.236927
Regulatory T cells limit vascular endothelial injury and prevent pulmonary hypertension
Abstract
Rationale: Pulmonary arterial hypertension (PAH) is an incurable disease associated with viral infections and connective tissue diseases. The relationship between inflammation and disease pathogenesis in these disorders remains poorly understood.
Objective: To determine whether immune dysregulation due to absent T-cell populations directly contributes to the development of PAH.
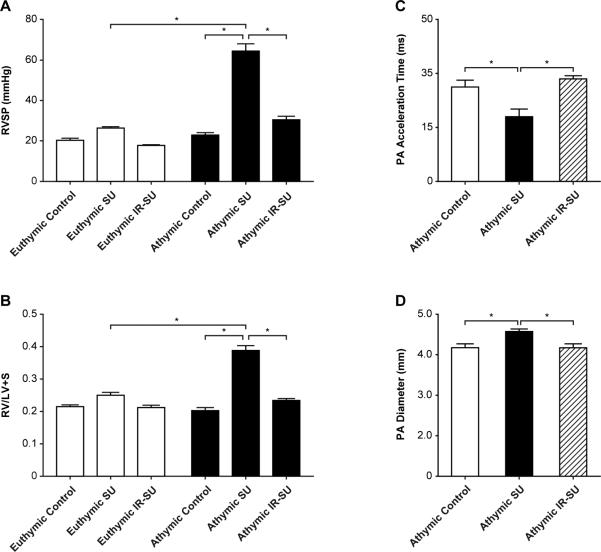
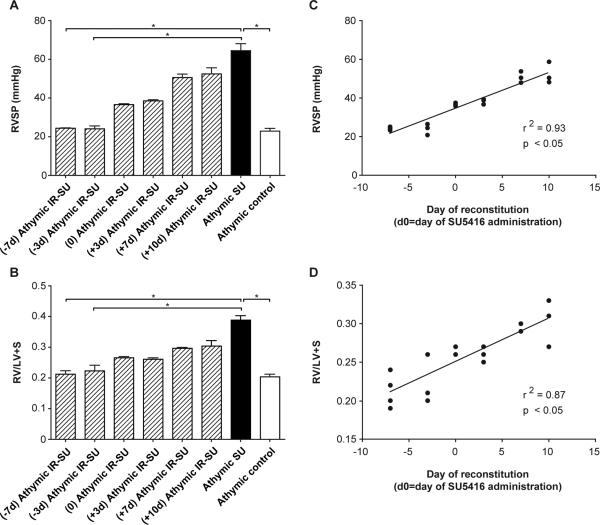
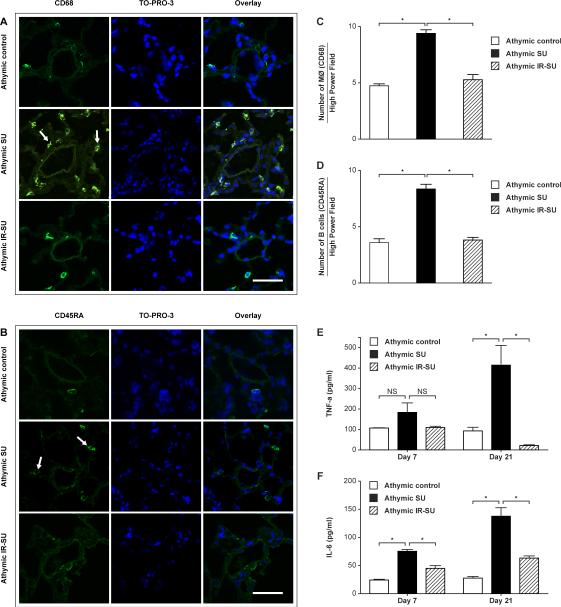
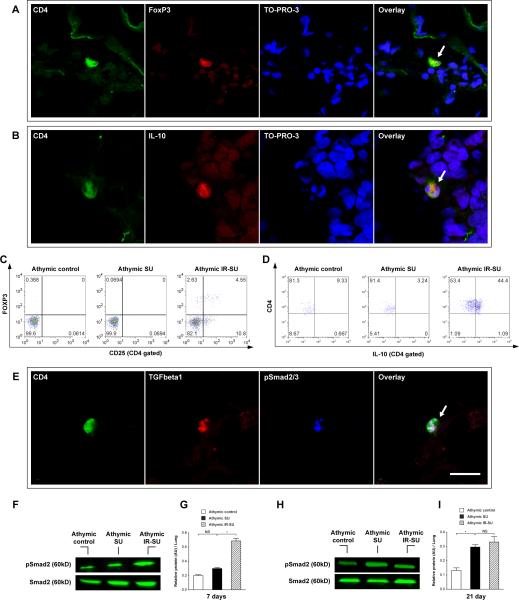
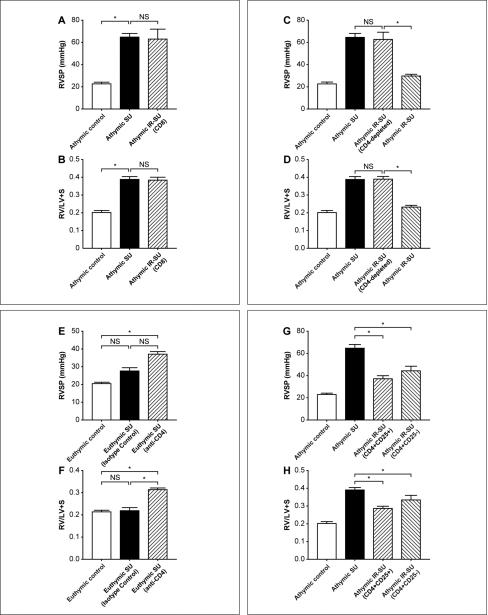
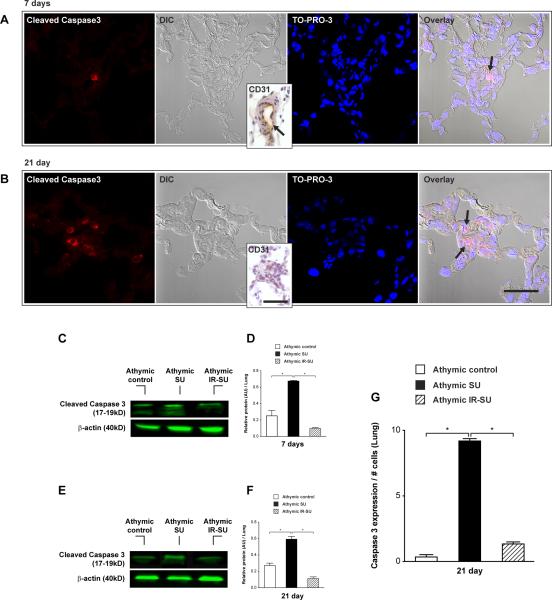
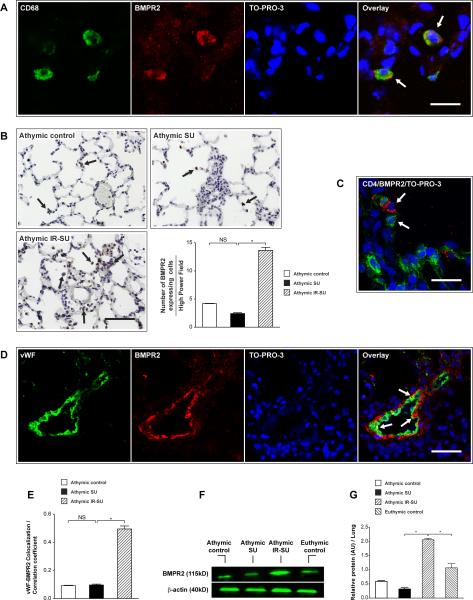
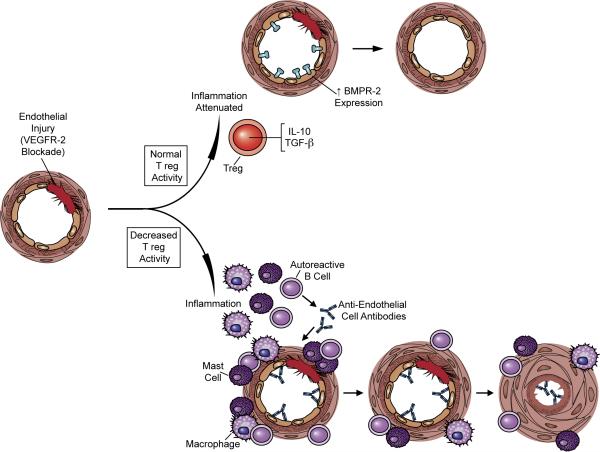
Methods and results: Vascular endothelial growth factor receptor 2 (VEGFR2) blockade induced significant pulmonary endothelial apoptosis in T-cell-deficient rats but not in immune-reconstituted (IR) rats. T cell-lymphopenia in association with VEGFR2 blockade resulted in periarteriolar inflammation with macrophages, and B cells even prior to vascular remodeling and elevated pulmonary pressures. IR prevented early inflammation and attenuated PAH development. IR with either CD8 T cells alone or with CD4-depleted spleen cells was ineffective in preventing PAH, whereas CD4-depleting immunocompetent euthymic animals increased PAH susceptibility. IR with either CD4(+)CD25(hi) or CD4(+)CD25(-) T cell subsets prior to vascular injury attenuated the development of PAH. IR limited perivascular inflammation and endothelial apoptosis in rat lungs in association with increased FoxP3(+), IL-10- and TGF-β-expressing CD4 cells, and upregulation of pulmonary bone morphogenetic protein receptor type 2 (BMPR2)-expressing cells, a receptor that activates endothelial cell survival pathways.
Conclusions: PAH may arise when regulatory T-cell (Treg) activity fails to control endothelial injury. These studies suggest that regulatory T cells normally function to limit vascular injury and may protect against the development of PAH.
Figures
References
-
- Nicolls MR, Taraseviciene-Stewart L, Rai PR, Badesch DB, Voelkel NF. Autoimmunity and pulmonary hypertension: a perspective. Eur Respir J. 2005;26(6):1110–1118. - PubMed
-
- Tuder RM, Voelkel NF. Pulmonary hypertension and inflammation. J Lab Clin Med. 1998;132(1):16–24. - PubMed
-
- Dorfmuller P, Perros F, Balabanian K, Humbert M. Inflammation in pulmonary arterial hypertension. Eur Respir J. 2003;22(2):358–363. - PubMed
-
- Hassoun PM, Mouthon L, Barbera JA, Eddahibi S, Flores SC, Grimminger F, Jones PL, Maitland ML, Michelakis ED, Morrell NW, Newman JH, Rabinovitch M, Schermuly R, Stenmark KR, Voelkel NF, Yuan JX, Humbert M. Inflammation, growth factors, and pulmonary vascular remodeling. J Am Coll Cardiol. 2009;54(1 Suppl):S10–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
