

Prognosis and therapy when acute promyelocytic leukemia and other "good risk" acute myeloid leukemias occur as a therapy-related myeloid neoplasm
- PMID: 21869918
- PMCID: PMC3152454
- DOI: 10.4084/MJHID.2011.032
Prognosis and therapy when acute promyelocytic leukemia and other "good risk" acute myeloid leukemias occur as a therapy-related myeloid neoplasm
Abstract
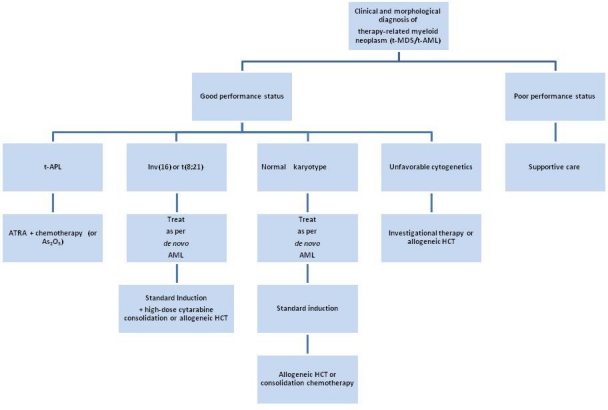
Treatment for a pre-existing condition using chemotherapy, radiation therapy, immunosuppressive therapy, or a combination of these modalities may lead to the devastating complication of therapy-related myelodysplastic syndrome or acute myeloid leukemia (t-MDS/t-AML), collectively known as therapy-related myeloid neoplasm (t-MN). This disorder arises as a direct consequence of mutational events induced by the primary treatment. The outcomes for these patients have been historically poor compared to people who develop AML de novo. Currently comprising 10-20% of all cases of AML, t-MN is relatively resistant to conventional leukemia therapies, and is associated with s ort survival times. Median life expectancy from diagnosis is about 8-10 months in most series. Although the spectrum of cytogenetic abnormalities in t-AML is similar to AML de novo, the frequency of unfavorable cytogenetics, such as a complex karyotype or deletion or loss of chromosomes 5 and/or 7, is considerably higher in t-MN. Two distinct groups of patients with t-MN have been described. The more common subtype, seen in about 75% of patients, typically occurs 5-7 years after first exposure to alkylating agents or radiation, is often preceded by a myelodysplastic syndrome (MDS), and is frequently accompanied by clonal cytogenetic abnormalities such as the loss of all or part of chromosomes 5 or 7. Mutations of the P53 tumor suppressor gene are also common. The risk is related to total cumulative exposure over time to alkylating agents. In contrast, among individuals who develop t-AML after treatment with topoisomerase II inhibitors, the latency period to the development of t-AML is often only 1-3 years, antecedent MDS is rare, and gene rearrangements involving MLL at 11q23 or RUNX1/AML1 at 21q22 are common. It is now well recognized that APL and other subtypes of AML with balanced translocations sometimes occur as therapy-related myeloid neoplasms (t-MN) in patients who have previously received cytotoxic therapy or ionizing radiation therapy (RT). The most of this review will focus on these "good risk" leukemias, i.e. those with APL or inv(16)/t(16;16) or t(8;21).
References
-
- Andersen MK, Johansson B, Larsen SO, Pedersen-Bjergaard J. Chromosomal abnormalities in secondary MDS and AML. Relationship to drugs and radiation with specific emphasis on the balanced rearrangements. Haematologica. 1998;83:483–488. - PubMed
-
- Larson RA, Le Beau MM, Ratain MJ, Rowley JD. Balanced translocations involving chromosome bands 11q23 and 21q22 in therapy-related leukemia. Blood. 1992;79:1892–1893. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous