

Augmented therapeutic efficacy of irinotecan is associated with enhanced drug accumulation
- PMID: 21872389
- PMCID: PMC3183362
- DOI: 10.1016/j.canlet.2011.07.023
Augmented therapeutic efficacy of irinotecan is associated with enhanced drug accumulation
Abstract
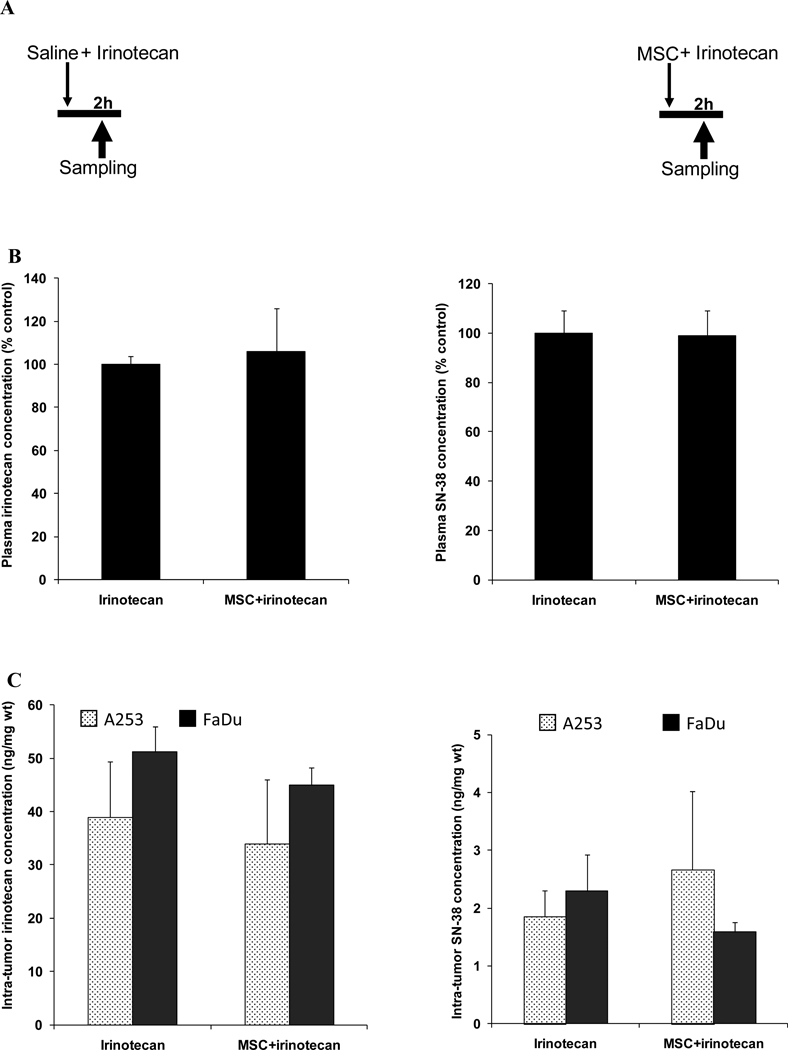
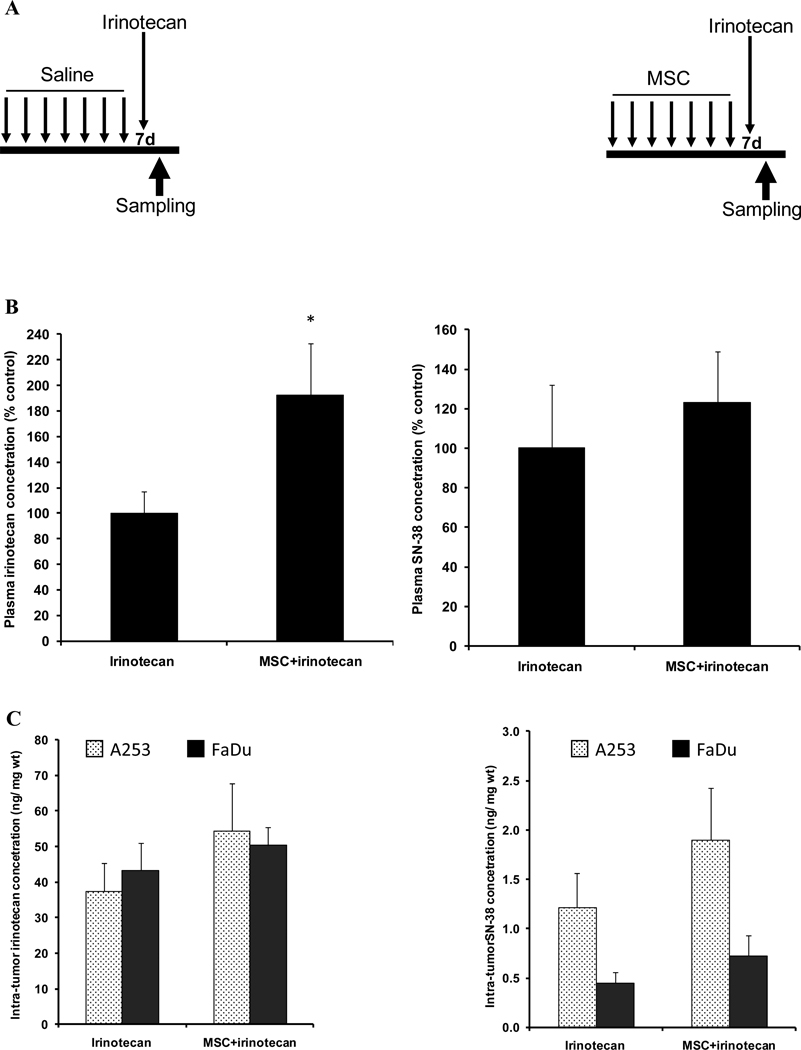
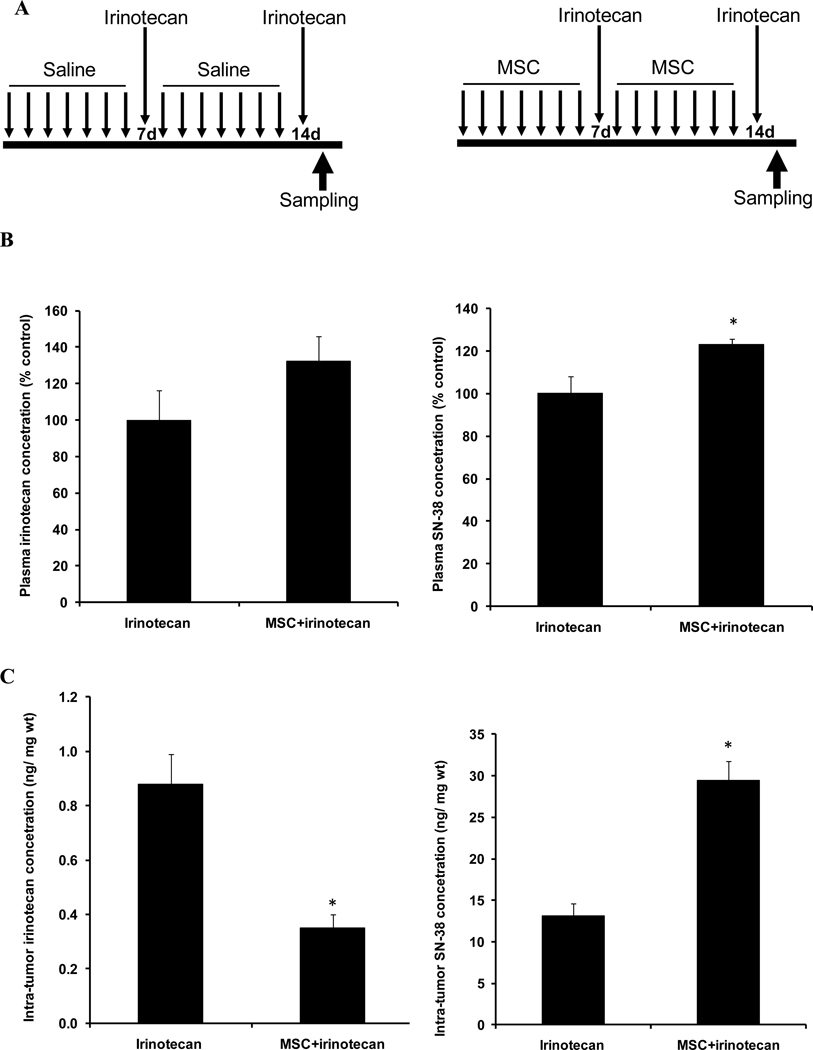
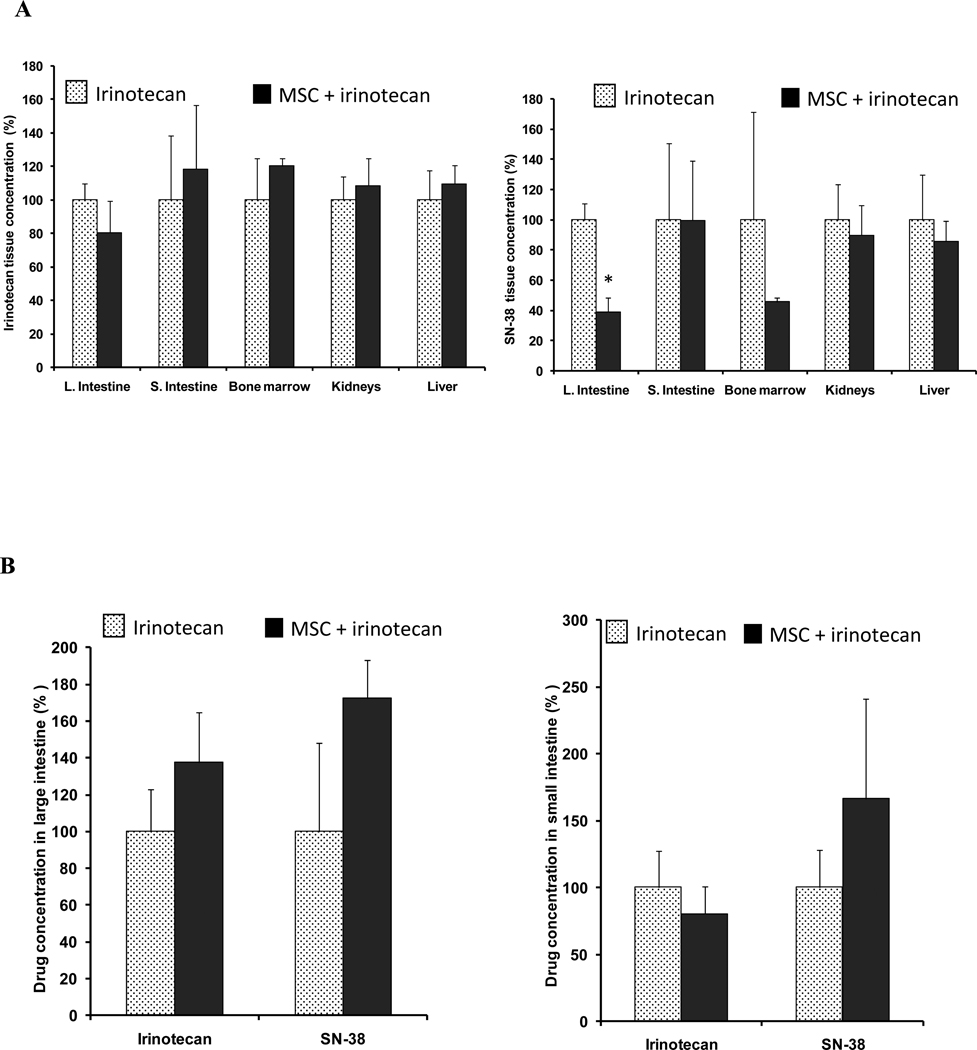
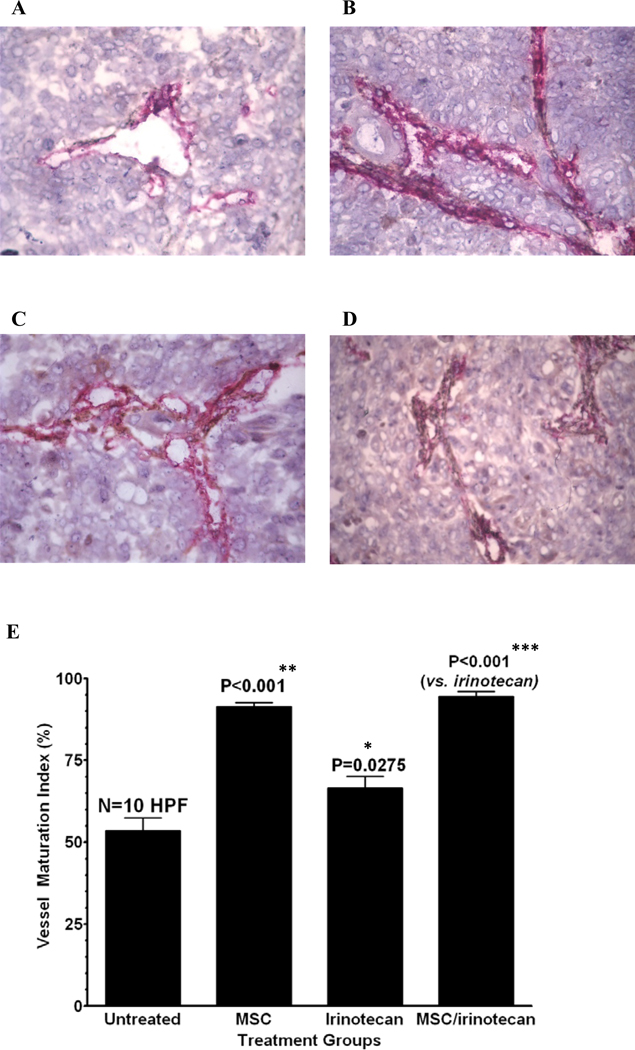
The goal of this study is to determine whether treatment with methylselenocysteine (MSC) results in differential uptake of irinotecan and its active metabolite (SN-38) between tumors of head and neck squamous cell carcinomas and normal tissue. The in vivo synergy between MSC and irinotecan is influenced by treatment schedule and associated with enhancement of tumor vessel maturation, intra-tumor concentration of SN-38 and apoptotic death of tumor cells. Normal tissue drug concentrations were not impacted by selenium treatment. The finding is of clinical relevance for enabling the delivery of higher doses of irinotecan to reverse tumor resistance, recurrence and ultimately enhancing cure rates.
Copyright © 2011 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
None of the authors has any financial or personal conflict of interest.
Figures

References
-
- Rivory LP, Bowles MR, Robert J, Pond SM. Conversion of irinotecan (CPT-11) to its active metabolite, 7-ethyl-10-hydroxycamptothecin (SN-38), by human liver carboxylesterase. Biochemical Pharmacology. 1996;52:1103–1111. - PubMed
-
- Ma MK, McLeod HL. Lessons learned from the irinotecan metabolic pathway. Current Medicinal Chemistry. 2003;10:41–49. - PubMed
-
- Rivory LP. Irinotecan (CPT-11): a brief overview. Clinical & Experimental Pharmacology & Physiology. 1996;23:1000–1004. - PubMed
-
- Ip C. Lessons from basic research in selenium and cancer prevention. Journal of Nutrition. 1998;128:1845–1854. - PubMed
-
- Cao S, Durrani F, Rustum YM. Selective modulation of the therapeutic efficacy of anticancer drugs by selenium containing compounds against human tumor xenografts. Clinical Cancer Resreach. 2004;10:2561–2569. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
