

Primary hyperaldosteronism: expanding the diagnostic net
- PMID: 21872791
- PMCID: PMC10832666
- DOI: 10.1016/j.jfms.2011.07.017
Primary hyperaldosteronism: expanding the diagnostic net
Abstract
Practical relevance: Primary hyperaldosteronism is probably the most common adrenocortical disorder in cats. As in humans, it is often unrecognised, which excludes a potentially large number of cats from appropriate treatment.
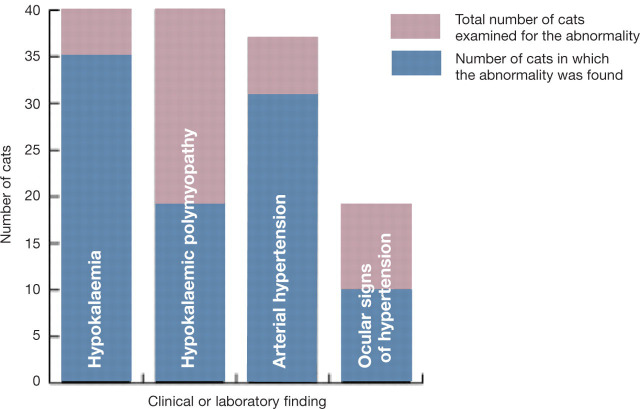
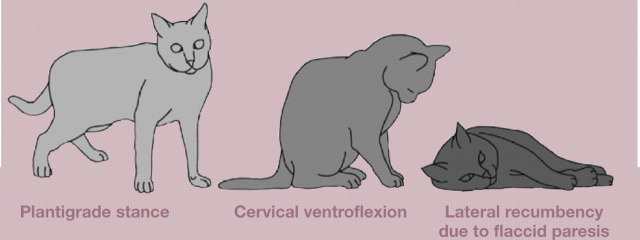
Patient group: Affected cats present at a median age of 13 years (range 5-20 years). A breed or sex predilection has not been documented. The excessive secretion of mineralocorticoids usually leads to hypokalaemia and/or systemic arterial hypertension. Most affected cats present with muscular weakness and/or ocular signs of arterial hypertension.
Diagnostics: In any cat presenting with hypokalaemia and/or arterial hypertension, other potential causes should be excluded. The ratio of plasma aldosterone concentration to plasma renin activity (aldosterone:renin ratio) is currently the best screening test for feline primary hyperaldosteronism. Diagnostic imaging is required to differentiate between adrenocortical neoplasia and bilateral hyperplasia, and to detect any distant metastases.
Clinical challenges: The differentiation between adrenocortical neoplasia and bilateral hyperplasia is imperative for planning optimal therapy, but the limited sensitivity of diagnostic imaging may occasionally pose a problem. For confirmed unilateral primary hyperaldosteronism, unilateral adrenalectomy is the treatment of choice, and offers an excellent prognosis, but potentially fatal intra- and postoperative haemorrhage is a reported complication and risk factors have yet to be identified.
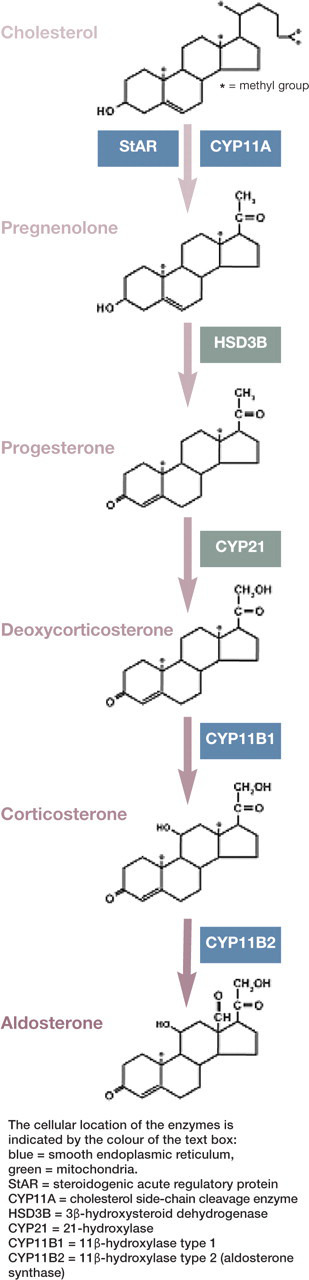
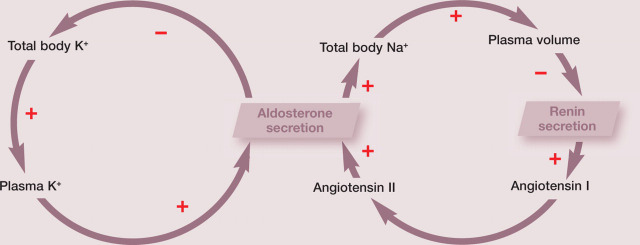
Evidence base: Only a few case reports are available on which to base the optimal diagnostic and therapeutic approach to feline primary hyperaldosteronism. This article reviews the physiology of aldosterone production and the pathophysiology of primary hyperaldosteronism, and summarises the currently available literature on the feline disease. Practical suggestions are given for the diagnostic investigation of cats with suspected primary hyperaldosteronism.
Copyright © 2011 ISFM and AAFP. Published by Elsevier Ltd. All rights reserved.
Figures




References
-
- Galac S, Reusch CE, Kooistra HS, Rijnberk A. Adrenals. In: Rijnberk A, Kooistra HS, eds. Clinical endocrinology of dogs and cats. 2nd edn. Hannover: Schlütersche, 2010: 93–154.
-
- Conn JW. Primary aldosteronism, a new clinical syndrome. J Lab Clin Med 1955; 45: 3–17. - PubMed
-
- Conn JW. The evolution of primary aldosteronism: 1954–1967. Harvey Lect 1966–1967; 62: 257–91. - PubMed
-
- Kaplan NM. Hypokalemia in the hypertensive patient, with observations on the incidence of primary aldosteronism. Ann Intern Med 1967; 66: 1079–90. - PubMed
-
- Fogari R, Preti P, Zoppi A, Rinaldi A, Fogari E, Mugellini A. Prevalence of primary aldosteronism among unselected hypertensive patients: a prospective study based on the use of an aldosterone/renin ratio above 25 as a screening test. Hypertens Res 2007; 30: 111–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
