

Brain abscess in seven cats due to a bite wound: MRI findings, surgical management and outcome
- PMID: 21872794
- PMCID: PMC7130018
- DOI: 10.1016/j.jfms.2011.07.020
Brain abscess in seven cats due to a bite wound: MRI findings, surgical management and outcome
Abstract
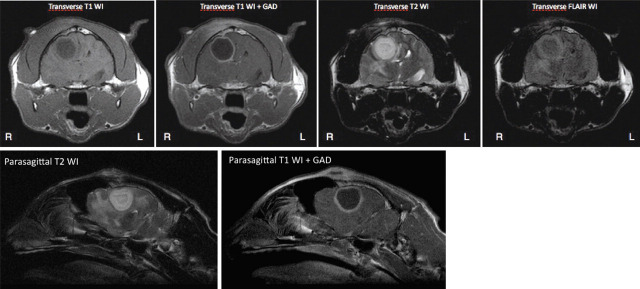
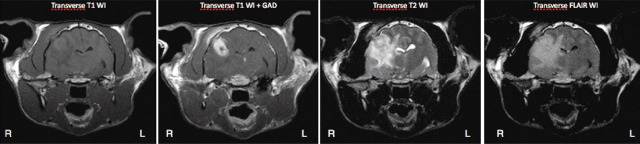
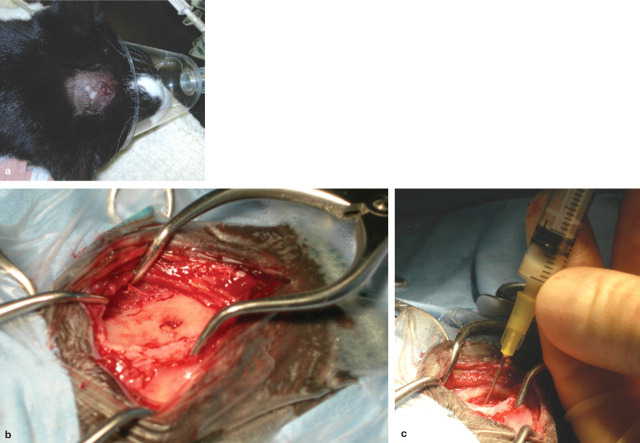
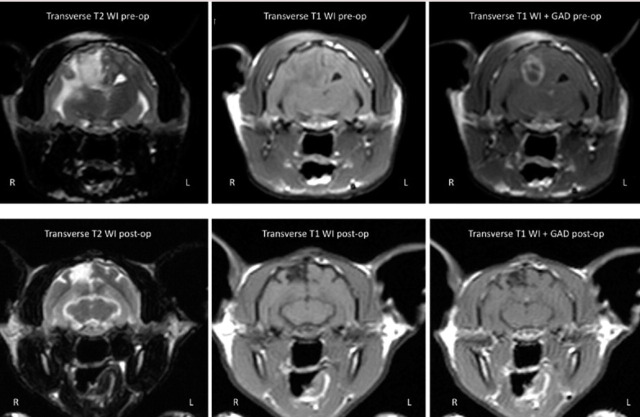
PRESENTATION AND LESION LOCALISATION: Seven adult domestic shorthair cats were presented with a 1- to 6-day history of progressive neurological signs. A focal skin puncture and subcutaneous swelling over the dorsal part of the head were detected on physical examination. Neurological examination indicated lesion(s) in the right forebrain in four cats, multifocal forebrain in one cat, left forebrain in one cat, and multifocal forebrain and brainstem in the remaining cat. In all cats, magnetic resonance imaging revealed a space-occupying forebrain lesion causing a severe mass effect on adjacent brain parenchyma. CLINICAL APPROACH AND OUTCOME: All cats were managed with a combination of medical and surgical treatment. At surgery a small penetrating calvarial fracture was detected in all cats, and a tooth fragment was found within the content of the abscess in two cats. The combination of surgical intervention, intensive care and intravenous antimicrobials led to a return to normal neurological function in five cats.
Practical relevance: As this series of cases indicates, successful resolution of a brain abscess due to a bite injury depends on early recognition and combined used of antimicrobials and surgical intervention. A particular aim of surgery is to remove any skull and foreign body (tooth) fragments that may represent a continuing focus of infection.
Copyright © 2011 ISFM and AAFP. All rights reserved.
Figures
References
-
- Roos K. Nonviral infections In: Goetz C, Pappert E, eds. Textbook of clinical neurology. Philadelphia: WB Saunders, 2000; 842–67.
-
- Sturges BK, Dickinson PJ, Kortz GD, et al. Clinical signs, magnetic resonance imaging features, and outcome after surgical and medical treatment of otogenic intracranial infection in 11 cats and 4 dogs. J Vet Intern Med 2006; 20: 648–56. - PubMed
-
- Barrs VR, Nicoll RG, Churcher RK, Beck JA, Beatty JA. Intracranial empyema: literature review and two novel cases in cats. J Small Anim Pract 2007; 48: 449–54. - PubMed
-
- Mateo I, Lorenzo V, Muñoz A, Pumarola M. Brainstem abscess due to plant foreign body in a dog. J Vet Intern Med 2007; 21: 535–38. - PubMed
-
- Bach JF, Mahony OM, Tidwell AS, Rush JE. Brain abscess and bacterial endocarditis in a Kerry Blue Terrier with a history of immune-mediated thrombocytopenia. J Vet Emerg Crit Care 2007; 17: 409–15.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
