

Genetic risk prediction in complex disease
- PMID: 21873261
- PMCID: PMC3179379
- DOI: 10.1093/hmg/ddr378
Genetic risk prediction in complex disease
Abstract
Attempting to classify patients into high or low risk for disease onset or outcomes is one of the cornerstones of epidemiology. For some (but by no means all) diseases, clinically usable risk prediction can be performed using classical risk factors such as body mass index, lipid levels, smoking status, family history and, under certain circumstances, genetics (e.g. BRCA1/2 in breast cancer). The advent of genome-wide association studies (GWAS) has led to the discovery of common risk loci for the majority of common diseases. These discoveries raise the possibility of using these variants for risk prediction in a clinical setting. We discuss the different ways in which the predictive accuracy of these loci can be measured, and survey the predictive accuracy of GWAS variants for 18 common diseases. We show that predictive accuracy from genetic models varies greatly across diseases, but that the range is similar to that of non-genetic risk-prediction models. We discuss what factors drive differences in predictive accuracy, and how much value these predictions add over classical predictive tests. We also review the uses and pitfalls of idealized models of risk prediction. Finally, we look forward towards possible future clinical implementation of genetic risk prediction, and discuss realistic expectations for future utility.
Figures
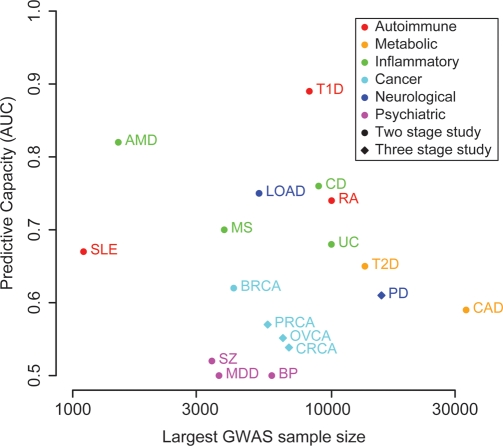
 , adjusted for the number of stages in the study (three stage studies have a smaller fraction of samples with GWAS data, and thus have lower power). Risk prediction is performed using logistic regression evaluated on data sets simulated from allele frequencies and odds ratios taken from replication data. PD: Parkinson's disease (45,46), AMD, age-related macular degeneration (47); T1D, type 1 diabetes (11); T2D, type 2 diabetes (48); UC, ulcerative colitis (49); CD, Crohn's disease (18,50); RA, rheumatoid arthritis (51); CAD, coronary artery disease (52); BRCA, breast cancer (53); LOAD, late-onset Alzheimer's disease (54,55); MS, multiple sclerosis (56); MDD, major depressive disorder (57); BP, bipolar disorder (58); SLE, systemic lupus erythematosus (59); SZ, schizophrenia (29); CRCA, colorectal cancer (60); PRCA, prostate cancer (61); OVCA, ovarian cancer (62,63).
, adjusted for the number of stages in the study (three stage studies have a smaller fraction of samples with GWAS data, and thus have lower power). Risk prediction is performed using logistic regression evaluated on data sets simulated from allele frequencies and odds ratios taken from replication data. PD: Parkinson's disease (45,46), AMD, age-related macular degeneration (47); T1D, type 1 diabetes (11); T2D, type 2 diabetes (48); UC, ulcerative colitis (49); CD, Crohn's disease (18,50); RA, rheumatoid arthritis (51); CAD, coronary artery disease (52); BRCA, breast cancer (53); LOAD, late-onset Alzheimer's disease (54,55); MS, multiple sclerosis (56); MDD, major depressive disorder (57); BP, bipolar disorder (58); SLE, systemic lupus erythematosus (59); SZ, schizophrenia (29); CRCA, colorectal cancer (60); PRCA, prostate cancer (61); OVCA, ovarian cancer (62,63).
References
-
- Lu K., Kauff N., Powell C.B., Chen L.M., Cass I., Lancaster J., Karlan B., Berchuck A., Mutch D. ACOG Practice Bulletin No. 103: hereditary breast and ovarian cancer syndrome. Obstet. Gynecol. 2009;113:957–966. - PubMed
-
- Zhernakova A., van Diemen C.C., Wijmenga C. Detecting shared pathogenesis from the shared genetics of immune-related diseases. Nat. Rev. Genet. 2009;10:43–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
