

Clopidogrel discontinuation after acute coronary syndromes: frequency, predictors and associations with death and myocardial infarction--a hospital registry-primary care linked cohort (MINAP-GPRD)
- PMID: 21875855
- PMCID: PMC3184230
- DOI: 10.1093/eurheartj/ehr340
Clopidogrel discontinuation after acute coronary syndromes: frequency, predictors and associations with death and myocardial infarction--a hospital registry-primary care linked cohort (MINAP-GPRD)
Abstract
Aims: Adherence to evidence-based treatments and its consequences after acute myocardial infarction (MI) are poorly defined. We examined the extent to which clopidogrel treatment initiated in hospital is continued in primary care; the factors predictive of clopidogrel discontinuation and the hazard of death or recurrent MI.
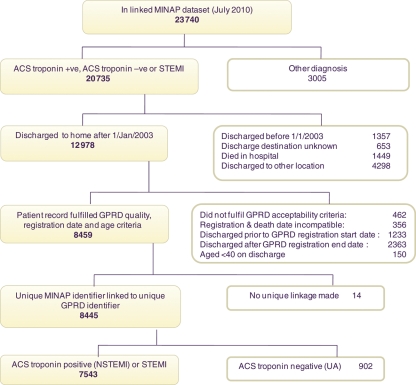
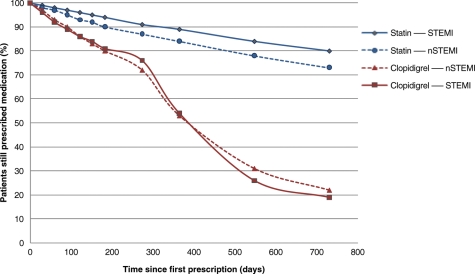
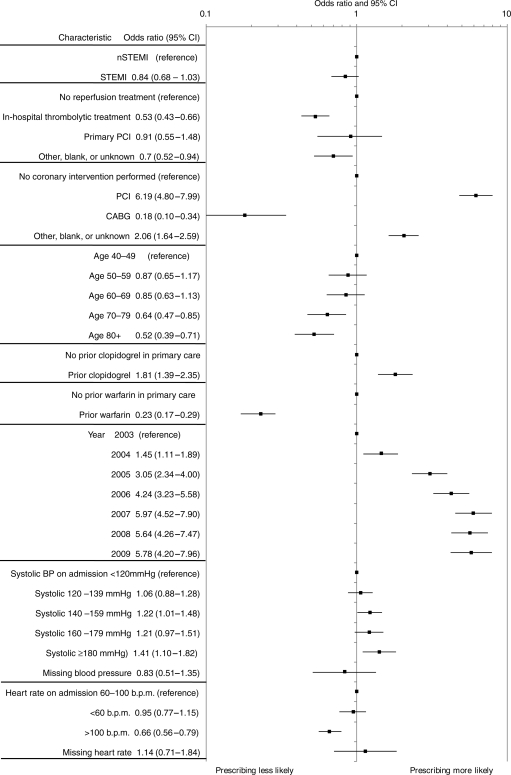
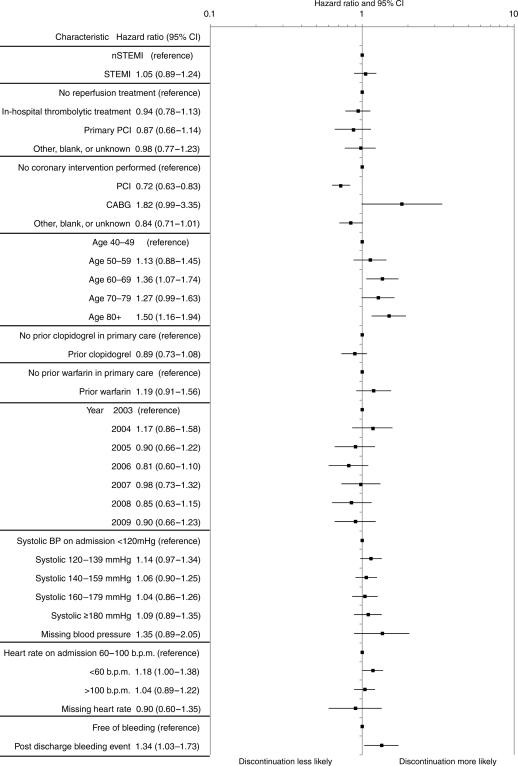
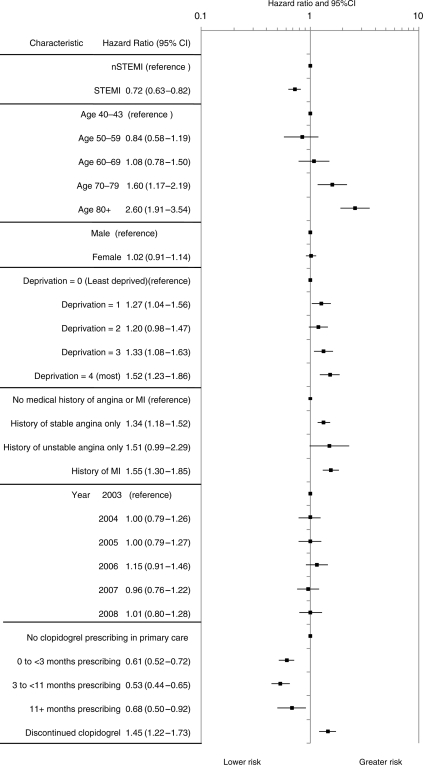
Methods and results: We linked the Myocardial Ischaemia National Audit Project registry and the General Practice Research Database to examine adherence to clopidogrel in primary care among patients discharged from hospital after MI (2003-2009). Hospital Episode Statistics and national mortality data were linked, documenting all-cause mortality and non-fatal MI. Of the 7543 linked patients, 4650 were prescribed clopidogrel in primary care within 3 months of discharge. The adjusted odds of still being prescribed clopidogrel at 12 months were similar following non-ST-elevation myocardial infarction (NSTEMI) 53% (95% CI, 51-55) and ST-elevation myocardial infarction (STEMI) 54% (95% CI, 52-56), but contrast with statins: NSTEMI 84% (95% CI, 82-85) and STEMI 89% (95% CI, 87-90). Discontinuation within 12 months was more frequent in older patients [>80 vs. 40-49 years, adjusted hazard ratio (HR) 1.50 (95% CI, 1.15-1.94)] and with bleeding events [HR 1.34 (95% CI, 1.03-1.73)]. 18.15 patients per 100 person-years (95% CI, 16.83-19.58) died or experienced non-fatal MI in the first year following discharge. In patients who discontinued clopidogrel within 12 months, the adjusted HR for death or non-fatal MI was 1.45 (95% CI, 1.22-1.73) compared with untreated patients, and 2.62 (95% CI, 2.17-3.17) compared with patients persisting with clopidogrel treatment.
Conclusion: This is the first study to use linked registries to determine persistence of clopidogrel treatment after MI in primary care. It demonstrates that discontinuation is common and associated with adverse outcomes.
Figures
References
-
- NICE Clinical Guideline 94. Unstable angina and NSTEMI. The early management of unstable angina and non-ST-segment-elevation myocardial infarction. 2010. March http://www.nice.org.uk/nicemedia/live/12949/47921/47921.pdf. (1 June 2011) - PubMed
-
- NICE Clinical Guideline 48. MI: secondary prevention. 2007. May http://www.nice.org.uk/nicemedia/live/11008/30497/30497.pdf. (1 June 2011)
-
- Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M. Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology. Eur Heart J. 2008;29:2909–2945. doi:10.1093/eurheartj/ehn526. - DOI - PubMed
-
- Bassand J-P, Hamm CW, Ardissino D, Boersma E, Budaj A, Hasdai D, Fernandez-Aviles F, Fox KAA, Ohman EM, Wallentin L, Wijns W. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur Heart J. 2007;28:1598–1660. doi:10.1093/eurheartj/ehm161. - DOI - PubMed
-
- Berger PB. Optimal duration of clopidogrel use after implantation of drug-eluting stents—still in doubt. N Engl J Med. 2010;362:1441–1443. doi:10.1056/NEJMe1002553. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
