

Pharmacokinetics of lopinavir/ritonavir crushed versus whole tablets in children
- PMID: 21876444
- PMCID: PMC3205189
- DOI: 10.1097/QAI.0b013e318232b057
Pharmacokinetics of lopinavir/ritonavir crushed versus whole tablets in children
Abstract
Objective: Lopinavir/ritonavir (Kaletra) is first-line therapy for pediatric HIV infection. In clinical practice, Kaletra tablets are occasionally crushed for pediatric administration. This study compared lopinavir/ritonavir exposure between whole and crushed tablets in HIV-infected children.
Design: This was a randomized, open-label, cross-over study of pediatric patients taking lopinavir/ritonavir as part of their antiretroviral regimen. Each subject had 2 separate (within 30 days) steady-state 12-hour pharmacokinetic (PK) studies with crushed and whole 200/50 mg lopinavir/ritonavir tablets.
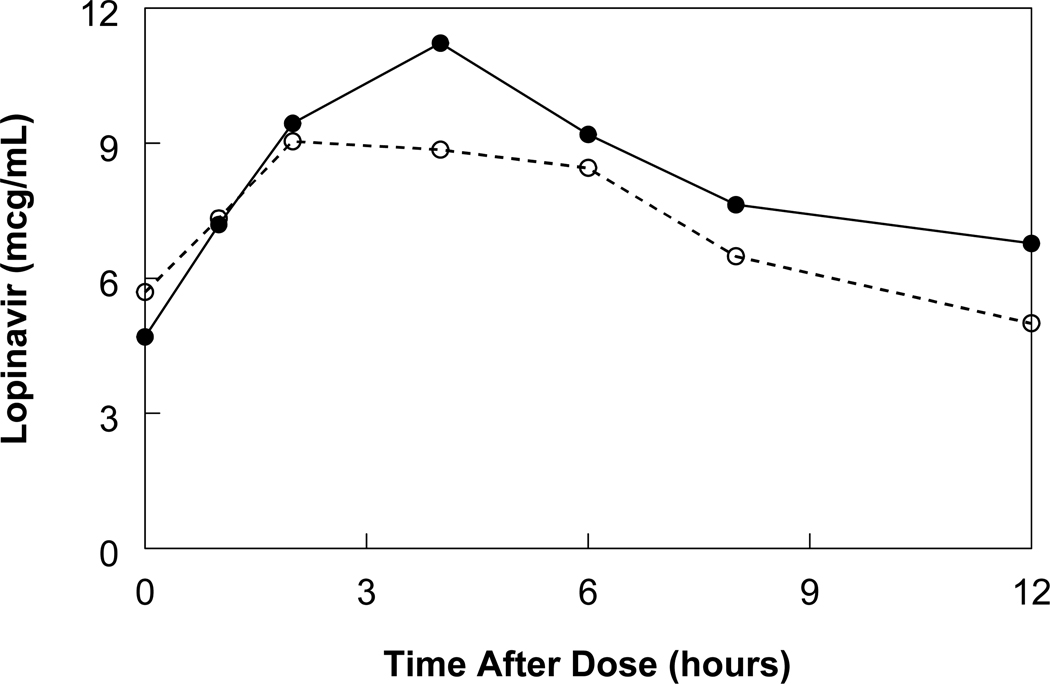
Methods: PK blood samples were drawn at 0 (predose), 1, 2, 4, 6, 8, and 12 hours postdose. Lopinavir and ritonavir plasma concentrations measured by high-performance liquid chromatography were used to calculate non-compartmental area under the concentration versus time curve (AUC) and clearance. Wilcoxon signed-rank tests compared PK values between crushed and whole tablets.
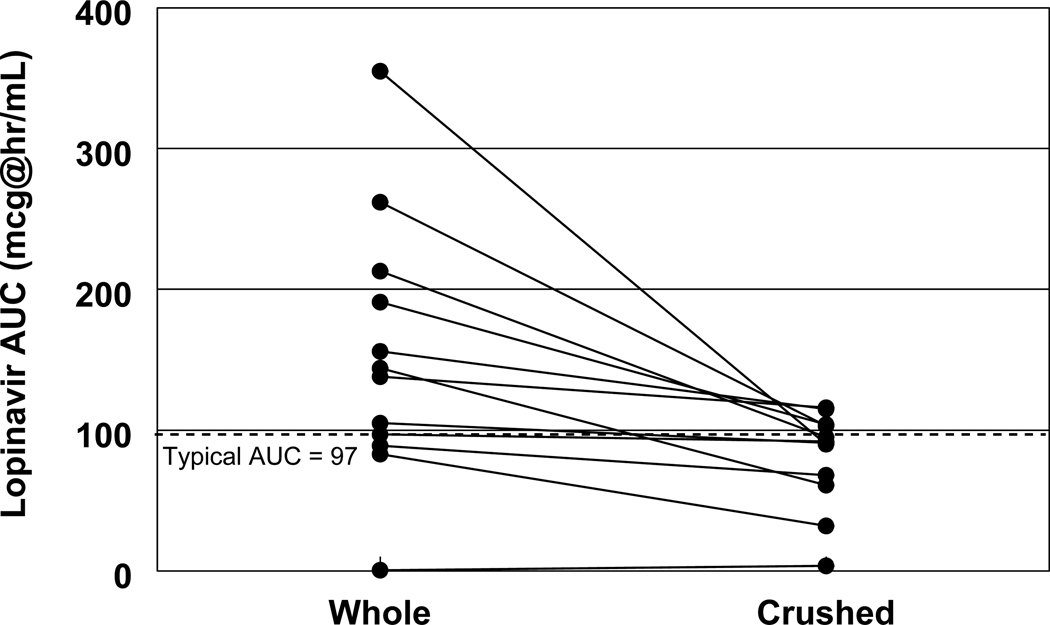
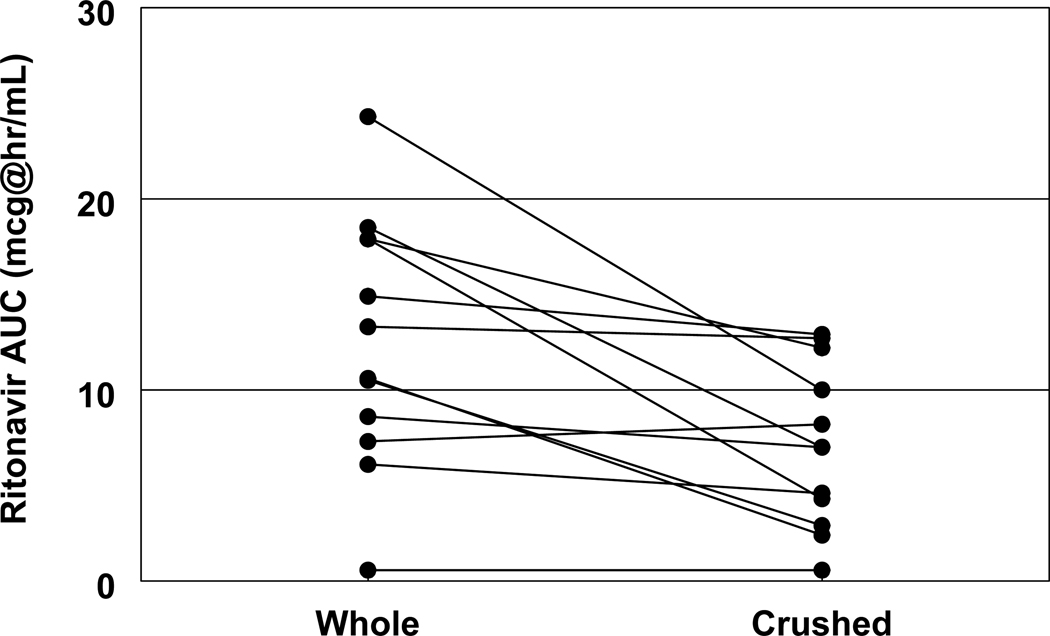
Results: Twelve children, median age of 13 years (10-16 years), took 550/138 mg·m(-2) per day lopinavir/ritonavir divided every 12 hours. The median lopinavir AUC after crushed and whole tablets were 92 mg·hr·L(-1) and 144 mg·hr·L(-1), respectively, with an AUC ratio of 0.55 (P = 0.003). Median ritonavir AUC of crushed and whole tablets were 7 mg·hr·L(-1) and 13.3 mg·hr·L(-1), respectively, with an AUC ratio of 0.53 (P = 0.006).
Conclusions: Administration of crushed 200/50 mg lopinavir/ritonavir tablets to children significantly reduced lopinavir and ritonavir exposure with a decrease in AUC by 45% and 47%, respectively. The administration of crushed tablets would require higher doses and therapeutic drug monitoring to ensure adequate lopinavir exposure in patients requiring this practice. The use of crushed lopinavir/ritonavir tablets should be avoided, if possible.
Conflict of interest statement
Figures

References
-
- World Health Organization. Geneva: WHO; 2010. Antiretroviral therapy of HIV Infection in infants and children: towards universal access: recommendations for a public health approach-2010 revision. - PubMed
-
- Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children. [Accessed January 01, 2011];Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Updated August 16, 2010. Available at http://aidsinfo.nih.gov/contentfiles/PediatricGuidelines.pdf.
-
- Welch S, Sharland M, Lyall EG, et al. PENTA 2009 guidelines for the use of antiretroviral therapy in paediatric HIV-1 infection. HIV Med. 2009;10:591–613. - PubMed
-
- Boxwell D, Cao K, Lewis L, et al. Neonatal toxicity of Kaletra oral solution – LPV, ethanol or propylene glycol? [Poster #708]. Presented at: CROI 2011: 18th Conference on Retroviruses and Opportunistic Infections; Boston, MA, USA. 2011.
-
- Kaletra® product labeling. North Chicago, IL, USA: Abbott Laboratories; 2005.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
