

The potential cost-effectiveness of amblyopia screening programs
- PMID: 21877675
- PMCID: PMC3673536
- DOI: 10.3928/01913913-20110823-02
The potential cost-effectiveness of amblyopia screening programs
Abstract
Purpose: To estimate the incremental cost-effective-ness of amblyopia screening at preschool and kindergarten, the costs and benefits of three amblyopia screening scenarios were compared to no screening and to each other: (1) acuity/stereopsis (A/S) screening at kindergarten, (2) A/S screening at preschool and kindergarten, and (3) photoscreening at preschool and A/S screening at kindergarten.
Methods: A probabilistic microsimulation model of amblyopia natural history and response to treatment with screening costs and outcomes estimated from two state programs was programmed. The probability was calculated that no screening and each of the three interventions were most cost-effective per incremental quality-adjusted life year (QALY) gained and case avoided.
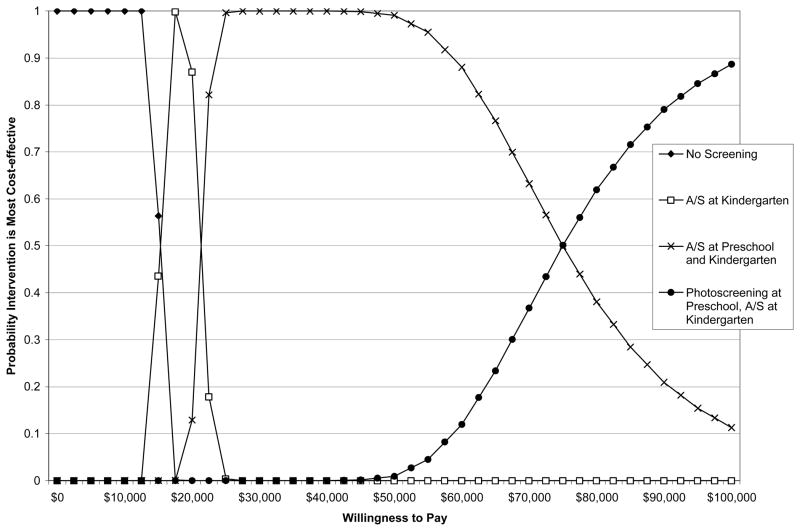
Results: Assuming a minimal 0.01 utility loss from monocular vision loss, no screening was most cost-effective with a willingness to pay (WTP) of less than $16,000 per QALY gained. A/S screening at kindergarten alone was most cost-effective at a WTP between $17,000 and $21,000. A/S screening at preschool and kindergarten was most cost-effective at a WTP between $22,000 and $75,000, and photoscreening at preschool and A/S screening at kindergarten was most cost-effective at a WTP greater than $75,000. Cost-effectiveness substantially improved when assuming a greater utility loss. All scenarios were cost-effective when assuming a WTP of $10,500 per case of amblyopia cured.
Conclusion: All three screening interventions evaluated are likely to be considered cost-effective relative to many other potential public health programs. The choice of screening option depends on budgetary resources and the value placed on monocular vision loss prevention by funding agencies.
Copyright 2012, SLACK Incorporated.
Conflict of interest statement
Conflict of Interest: No authors have any financial/conflicting interests to disclose.
Figures
References
-
- American Academy of Ophthalmology (AAO) Preferred practice pattern guidelines: Amblyopia. San Francisco, CA: American Academy of Ophthalmology; 2007.
-
- Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J. The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: A systematic review and economic evaluation. Health Technol Assess. 2008;12(25):1–214. - PubMed
-
- White A. Eye exams for children: Their impact and cost effectiveness. Cambridge, MA: Abt Associates; 2004. Prepared for the Vision Council of America.
-
- König HH, Barry JC. Cost-utility analysis of orthoptic screening in kindergarten: A Markov model based on data from Germany. Pediatrics. 2004;113(2):e95–108. - PubMed
-
- König HH, Barry JC, Leidl R, Zrenner E. Economic evaluation of orthoptic screening: Results of a field study in 121 German kindergartens. Invest Ophthalmol Vis Sci. 2002;43(10):3209–3215. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
