

Which factors influence preservation of the osteonecrotic femoral head?
- PMID: 21879405
- PMCID: PMC3254748
- DOI: 10.1007/s11999-011-2050-4
Which factors influence preservation of the osteonecrotic femoral head?
Abstract
Background: Although surgeons use many procedures to preserve the femoral head in patients with hip osteonecrosis, there is no consensus regarding the best procedure.
Questions/purposes: We raised the following questions: (1) Is one surgical treatment preferred based on published data? (2) What are the rates of radiographic progression or conversion to THA after treatment of pre- and postcollapse hips? (3) Does lesion size in the femoral head influence progression? And (4) does the extent of involvement of the weightbearing surface of the femoral head influence outcome?
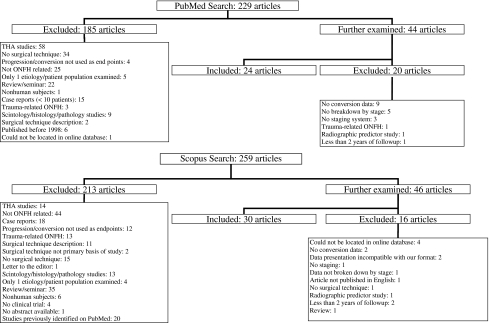
Methods: We searched MEDLINE and Scopus for articles published between 1998 and 2010. We included only articles assessing an operative intervention for hip osteonecrosis and having a level of evidence of I to IV. We included 54 of the 488 reviewed manuscripts.
Results: No procedure was superior to others. In pre- and postcollapse hips, 264 of 864 hips (31%) and 419 of 850 hips (49%), respectively, exhibited radiographic disease progression. There were lower failure rates when the lesion involved less than 15% of the femoral head or had a necrotic angle of less than 200° (14%-25%) and when the osteonecrotic lesion involved only the medial 1/3 of the weightbearing surface (4.6%).
Conclusions: The best treatment of precollapse lesions is difficult to determine due to the limitations of the available literature. However, the data suggest operative intervention prevents collapse of small lesions of the femoral head or when there is a limited amount of the weightbearing surface involved. Patients with head collapse have a high progression rate after a femoral head-saving procedure.
Figures
References
-
- Berend KR, Gunneson EE, Urbaniak JR. Free vascularized fibular grafting for the treatment of postcollapse osteonecrosis of the femoral head. J Bone Joint Surg Am. 2003;85:987–993. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
