

Prolonged survival with valproic acid use in the EORTC/NCIC temozolomide trial for glioblastoma
- PMID: 21880994
- PMCID: PMC3265044
- DOI: 10.1212/WNL.0b013e31822f02e1
Prolonged survival with valproic acid use in the EORTC/NCIC temozolomide trial for glioblastoma
Abstract
Objective: This analysis was performed to assess whether antiepileptic drugs (AEDs) modulate the effectiveness of temozolomide radiochemotherapy in patients with newly diagnosed glioblastoma.
Methods: The European Organization for Research and Treatment of Cancer (EORTC) 26981-22981/National Cancer Institute of Canada (NCIC) CE.3 clinical trial database of radiotherapy (RT) with or without temozolomide (TMZ) for newly diagnosed glioblastoma was examined to assess the impact of the interaction between AED use and chemoradiotherapy on survival. Data were adjusted for known prognostic factors.
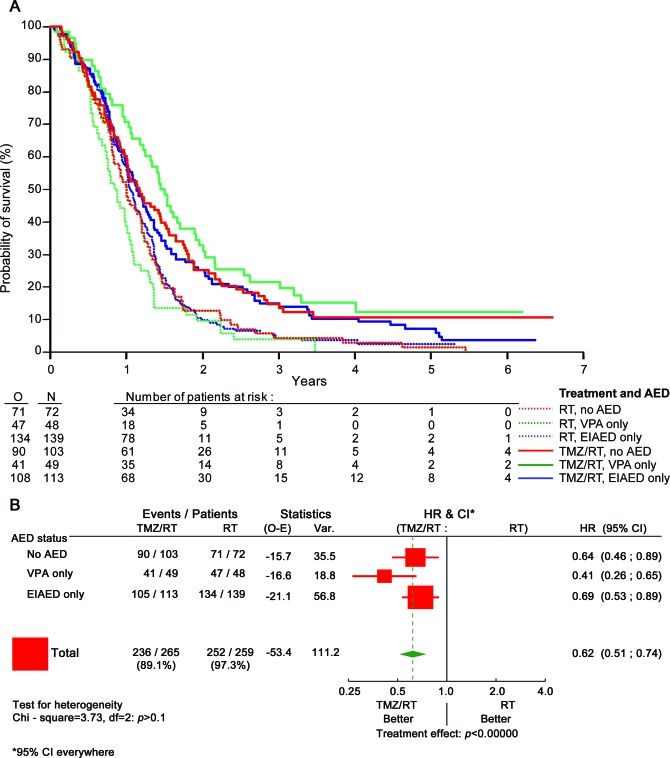
Results: When treatment began, 175 patients (30.5%) were AED-free, 277 (48.3%) were taking any enzyme-inducing AED (EIAED) and 135 (23.4%) were taking any non-EIAED. Patients receiving valproic acid (VPA) only had more grade 3/4 thrombopenia and leukopenia than patients without an AED or patients taking an EIAED only. The overall survival (OS) of patients who were receiving an AED at baseline vs not receiving any AED was similar. Patients receiving VPA alone (97 [16.9%]) appeared to derive more survival benefit from TMZ/RT (hazard ratio [HR] 0.39, 95% confidence interval [CI] 0.24-0.63) than patients receiving an EIAED only (252 [44%]) (HR 0.69, 95% CI 0.53-0.90) or patients not receiving any AED (HR 0.67, 95% CI 0.49-0.93).
Conclusions: VPA may be preferred over an EIAED in patients with glioblastoma who require an AED during TMZ-based chemoradiotherapy. Future studies are needed to determine whether VPA increases TMZ bioavailability or acts as an inhibitor of histone deacetylases and thereby sensitizes for radiochemotherapy in vivo.
Figures
Comment in
-
Valproic acid as the AED of choice for patients with glioblastoma? The jury is out.Neurology. 2011 Sep 20;77(12):1114-5. doi: 10.1212/WNL.0b013e31822f0325. Epub 2011 Aug 31. Neurology. 2011. PMID: 21880995 No abstract available.
References
-
- Van Breemen MS, Wilms EB, Vecht CJ. Epilepsy in patients with brain tumours: epidemiology, mechanisms, and management. Lancet Neurol 2007;6:421–430 - PubMed
-
- Wick W, Menn O, Meisner C, et al. Pharmacotherapy of epileptic seizures in glioma patients: who, when, why and how long? Onkologie 2005;28:391–396 - PubMed
-
- Glantz MJ, Cole BF, Forsyth PA, et al. Practice parameter: anticonvulsant prophylaxis in patients with newly diagnosed brain tumors: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000;54:1886–1893 - PubMed
-
- Bourg V, Lebrun C, Chichmanian RM, Thomas P, Frenay M. Nitroso-urea-cisplatin-based chemotherapy associated with valproate: increase of haematologic toxicity. Ann Oncol 2001;12:217–219 - PubMed
-
- Ward MM, Barbaro NM, Laxer KD, Rampil IJ. Preoperative valproate administration does not increase blood loss during temporal lobectomy. Epilepsia 1996;37:98–101 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical