

Pipeline embolization device (PED) for neurovascular reconstruction: initial experience in the treatment of 101 intracranial aneurysms and dissections
- PMID: 21881914
- PMCID: PMC3304061
- DOI: 10.1007/s00234-011-0948-x
Pipeline embolization device (PED) for neurovascular reconstruction: initial experience in the treatment of 101 intracranial aneurysms and dissections
Abstract
Introduction: The purpose of this study was to evaluate the safety and efficacy of the recently available flow diverter "pipeline embolization device" (PED) for the treatment of intracranial aneurysms and dissections.
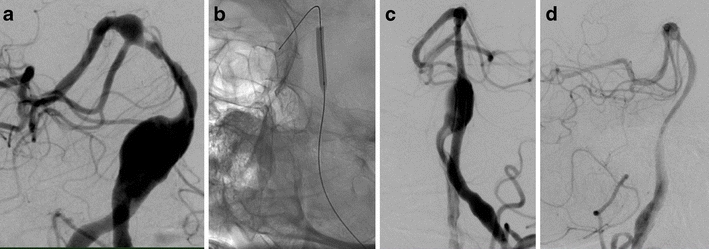
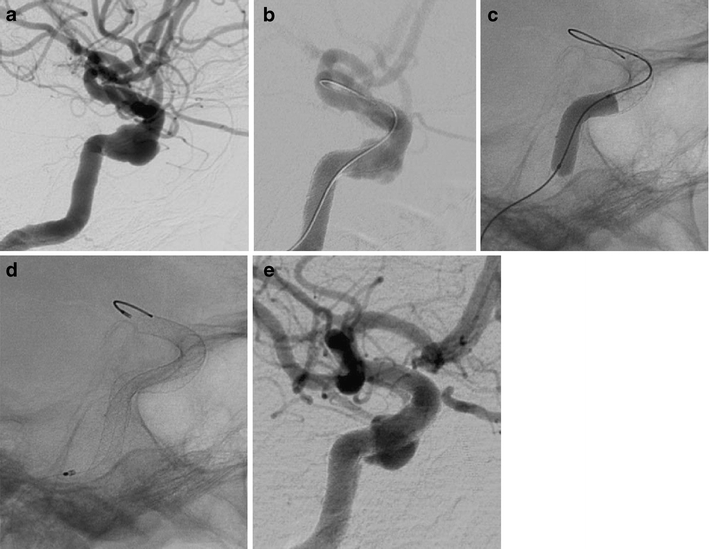
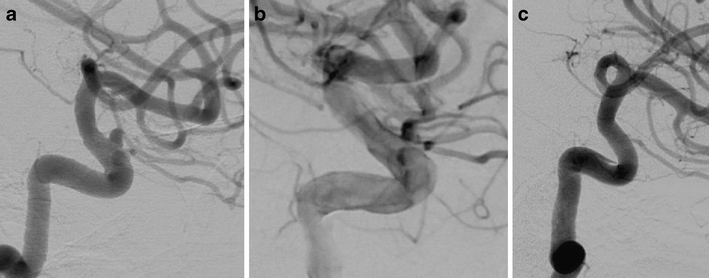
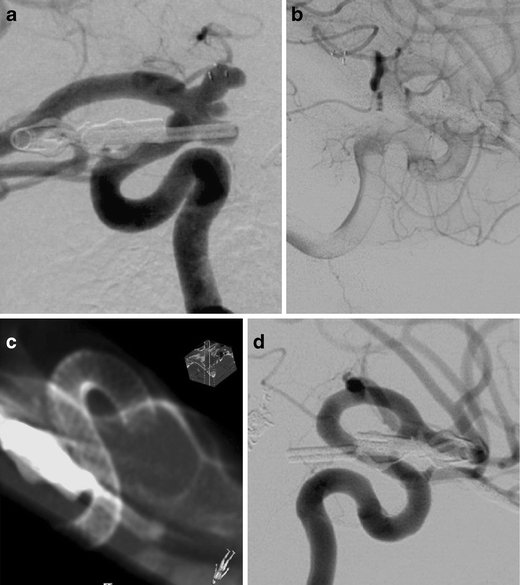
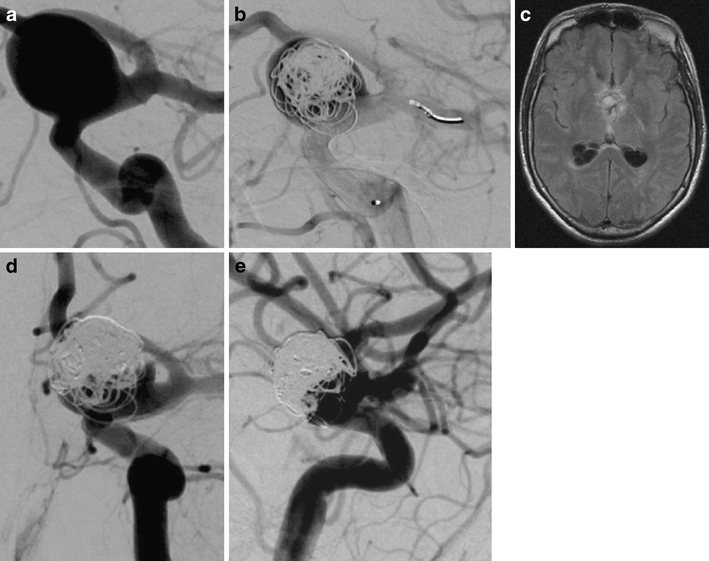
Methods: Eighty-eight consecutive patients underwent an endovascular treatment of 101 intracranial aneurysms or dissections using the PED between September 2009 and January 2011. The targeted vessels include 79 (78%) in the anterior circulation and 22 (22%) in the posterior circulation. We treated 96 aneurysms and 5 vessel dissections. Multiple devices were implanted in 67 lesions (66%).
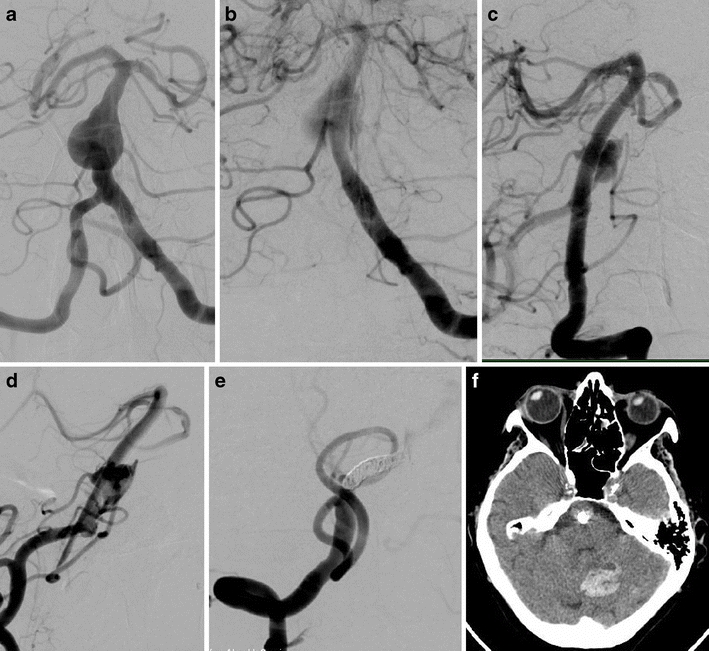
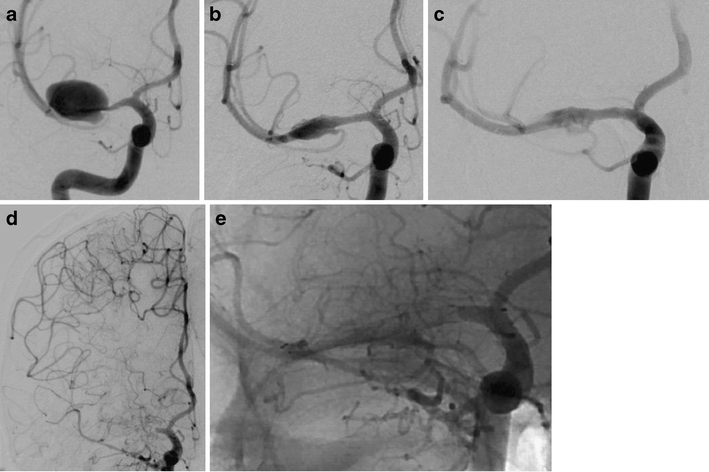
Results: One technical failure of the procedure was encountered. Immediate exclusion of the target lesion was not observed. Angiographic follow-up examinations were carried out in 80 patients (91%) with 90 lesions and revealed complete cure of the target lesion(s) in 47 (52%), morphological improvement in 32 lesions (36%), and no improvement in 11 lesions (12%). Six major complications were encountered: one fatal aneurysm rupture, one acute and one delayed PED thrombosis, and three hemorrhages in the dependent brain parenchyma.
Conclusion: Our experience reveals that the PED procedure is technically straightforward for the treatment of selected wide-necked saccular aneurysms, fusiform aneurysms, remnants of aneurysms, aneurysms with a high likelihood of failure with conventional endovascular techniques, and dissected vessels. While vessel reconstruction, performed after dissection, is achieved within days, remodeling of aneurysmal dilatations may take several months. Dual platelet inhibition is obligatory. Parenchymal bleeding into brain areas dependent on the target vessel is uncommon.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
