

Portal vein thrombosis is a potentially preventable complication in clinical islet transplantation
- PMID: 21883914
- PMCID: PMC3226916
- DOI: 10.1111/j.1600-6143.2011.03717.x
Portal vein thrombosis is a potentially preventable complication in clinical islet transplantation
Abstract
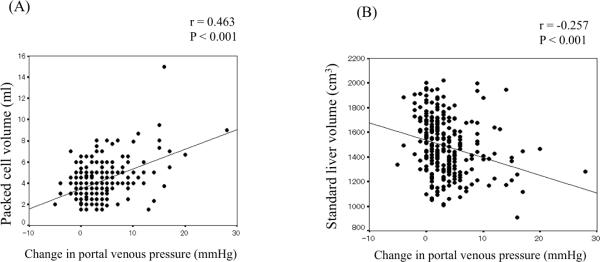
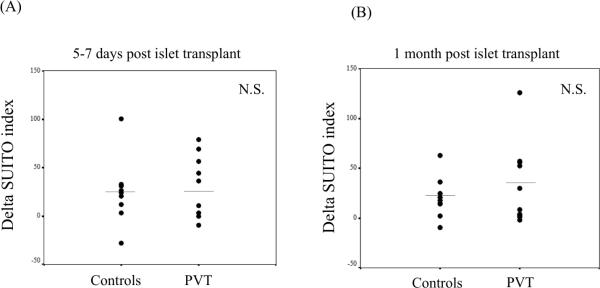
Percutaneous transhepatic portal access avoids surgery but is rarely associated with bleeding or portal venous thrombosis (PVT). We herein report our large, single-center experience of percutaneous islet implantation and evaluate risk factors of PVT and graft function. Prospective data were collected on 268 intraportal islet transplants (122 subjects). A portal venous Doppler ultrasound was obtained on Days 1 and 7 posttransplant. Therapeutic heparinization, complete ablation of the portal catheter tract with Avitene paste and limiting packed cell volume (PCV) to <5 mL completely prevented any portal thrombosis in the most recent 101 islet transplant procedures over the past 5 years. In the previous cumulative experience, partial thrombosis did not affect islet function. Standard liver volume correlated negatively (r =-0.257, p < 0.001) and PCV correlated positively with portal pressure rise (r = 0.463, p < 0.001). Overall, partial portal thrombosis occurred after 10 procedures (overall incidence 3.7%, most recent 101 patient incidence 0%). There were no cases of complete thrombosis and no patient developed sequelae of portal hypertension. In conclusion, portal thrombosis is a preventable complication in clinical islet transplantation, provided therapeutic anticoagulation is maintained and PCV is limited to <5 mL.
©Copyright 2011 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures



References
-
- Shapiro AM, Lakey JR, Ryan EA, Korbutt GS, Toth E, Warnock GL, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med. 2000;343(4):230–238. - PubMed
-
- Ricordi C, Strom TB. Clinical islet transplantation: advances and immunological challenges. Nat Rev Immunol. 2004;4(4):259–268. - PubMed
-
- Hering BJ, Kandaswamy R, Ansite JD, Eckman PM, Nakano M, Sawada T, et al. Single-donor, marginal-dose islet transplantation in patients with type 1 diabetes. JAMA. 2005;293(7):830–835. - PubMed
-
- Froud T, Yrizarry JM, Alejandro R, Ricordi C. Use of D-STAT to prevent bleeding following percutaneous transhepatic intraportal islet transplantation. Cell Transplant. 2004;13(1):55–59. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
