

Clinical and demographic predictors of outcomes in recent onset dilated cardiomyopathy: results of the IMAC (Intervention in Myocarditis and Acute Cardiomyopathy)-2 study
- PMID: 21884947
- PMCID: PMC6467576
- DOI: 10.1016/j.jacc.2011.05.033
Clinical and demographic predictors of outcomes in recent onset dilated cardiomyopathy: results of the IMAC (Intervention in Myocarditis and Acute Cardiomyopathy)-2 study
Erratum in
- J Am Coll Cardiol. 2011 Oct 18;58(17):1832
Abstract
Objectives: We sought to determine clinical and demographic predictors of recovery of left ventricular function for subjects with recent onset cardiomyopathy (ROCM).
Background: Although ROCM is a frequent reason for consultation and transplantation referral, its prognosis and natural history on contemporary therapy are unknown.
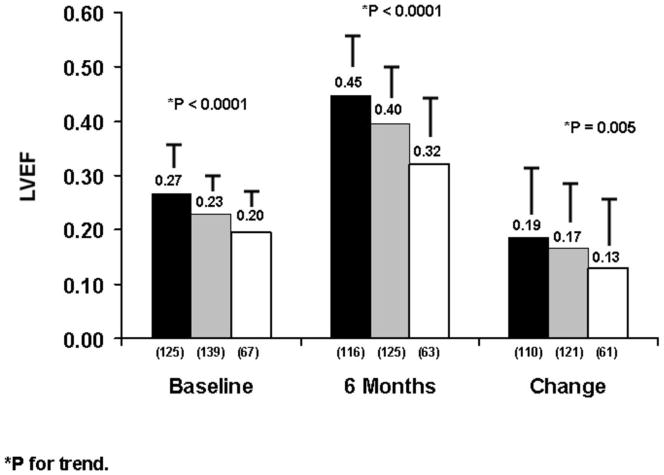
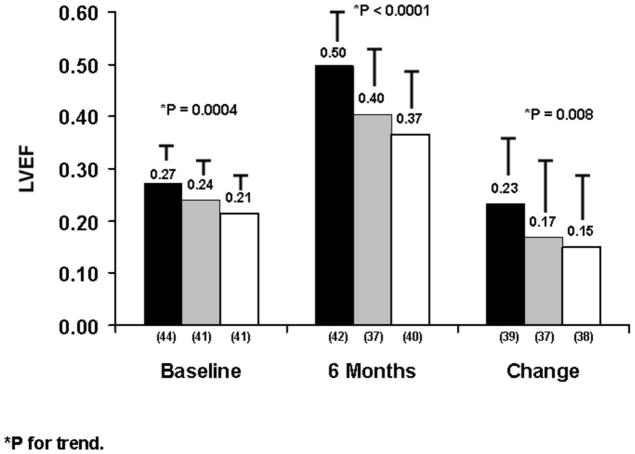
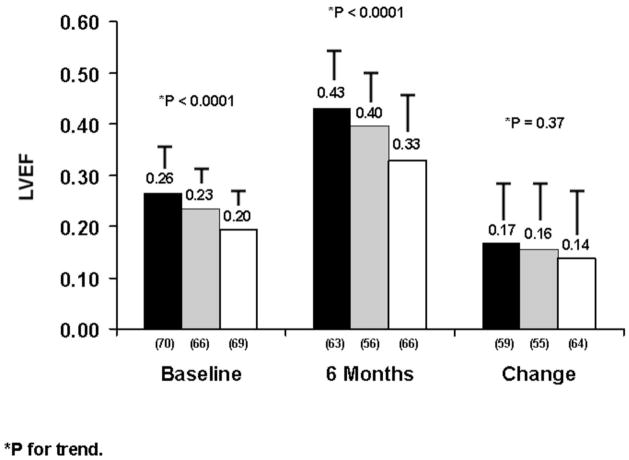
Methods: In the multicenter IMAC (Intervention in Myocarditis and Acute Cardiomyopathy)-2 study, subjects with a left ventricular ejection fraction (LVEF) of ≤0.40, fewer than 6 months of symptom duration, and an evaluation consistent with idiopathic dilated cardiomyopathy or myocarditis were enrolled. LVEF was reassessed at 6 months, and subjects were followed up for 4 years. LVEF and event-free survival were compared by race, sex, and clinical phenotype.
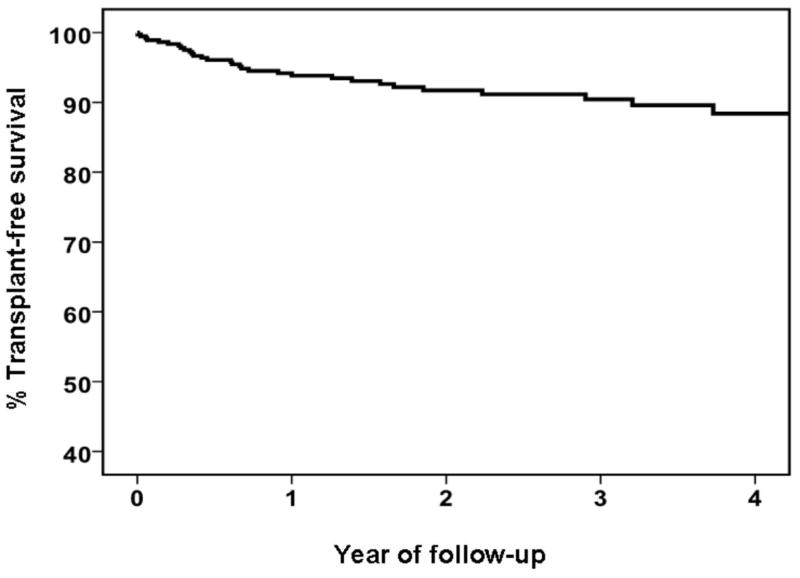
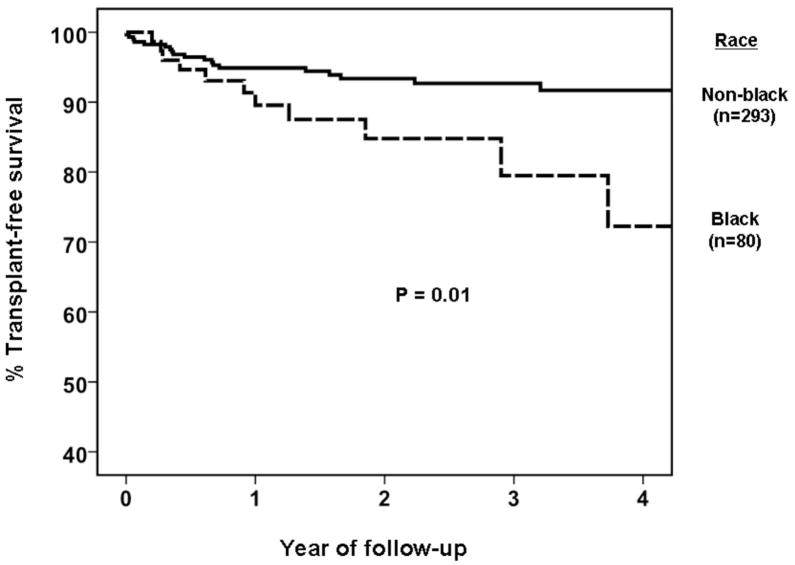
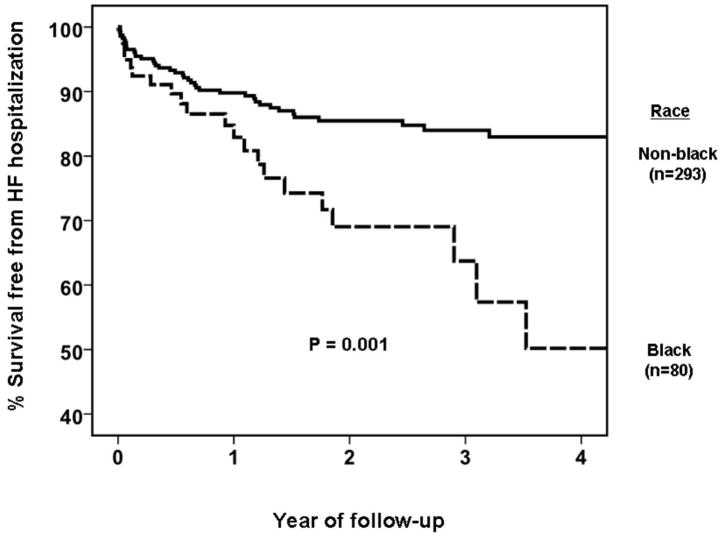
Results: The cohort of 373 persons was 38% female and 21% black, with a mean age of 45 ± 14 years. At entry, 91% were receiving angiotensin-converting enzyme inhibitors or angiotensin receptor blockers and 82% were receiving beta-blockers, which increased to 92% and 94% at 6 months. LVEF was 0.24 ± 0.08 at entry and 0.40 ± 0.12 at 6 months (mean increase: 17 ± 13 ejection fraction units). Transplant-free survival at 1, 2, and 4 years was 94%, 92%, and 88%, respectively; survival free of heart failure hospitalization was 88%, 82%, and 78%, respectively. In analyses adjusted for sex, baseline LVEF, and blood pressure, LVEF at 6 months was significantly lower in blacks than in nonblacks (p = 0.02). Left ventricular end-diastolic diameter at presentation was the strongest predictor of LVEF at 6 months (p < 0.0001).
Conclusions: Outcomes in ROCM are favorable but differ by race. Left ventricular end-diastolic diameter by transthoracic echo at presentation was most predictive of subsequent myocardial recovery. (Genetic Modulation of Left Ventricular Recovery in Recent Onset Cardiomyopathy; NCT00575211).
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
A new Era in the natural history of dilated cardiomyopathy.J Am Coll Cardiol. 2012 Feb 21;59(8):776; author reply 776-7. doi: 10.1016/j.jacc.2011.09.070. J Am Coll Cardiol. 2012. PMID: 22340272 No abstract available.
References
-
- Taylor DO, Stehlik J, Edwards LB, et al. Registry of the International Society for Heart and Lung Transplantation: Twenty-sixth Official Adult Heart Transplant Report-2009. J Heart Lung Transplant. 28:1007–1022. - PubMed
-
- Codd MB, Sugrue DD, Gersh BJ, Melton LJ., 3rd Epidemiology of idiopathic dilated and hypertrophic cardiomyopathy. A population-based study in Olmsted County, Minnesota, 1975–1984. Circulation. 1989 Sep;80(3):564–72. - PubMed
-
- Cooper LT, Virmani R, Chapman NM, et al. National Institutes of Health-sponsored workshop on inflammation and immunity in dilated cardiomyopathy. Mayo Clin Proc. 2006 Feb;81(2):199–204. - PubMed
-
- Dec GW, Palacios IF, Fallon JT, et al. Active myocarditis in the spectrum of acute dilated cardiomyopathies. N Engl J Med. 1985;312(14):885–890. - PubMed
-
- Parrillo JE, Cunnion RE, Epstein SE, et al. A prospective, randomized, controlled trial of prednisone for dilated cardiomyopathy. N Engl J Med. 1989;321:1061–1068. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
