

Noninvasive electroanatomic mapping of human ventricular arrhythmias with electrocardiographic imaging
- PMID: 21885406
- PMCID: PMC3182467
- DOI: 10.1126/scitranslmed.3002152
Noninvasive electroanatomic mapping of human ventricular arrhythmias with electrocardiographic imaging
Abstract
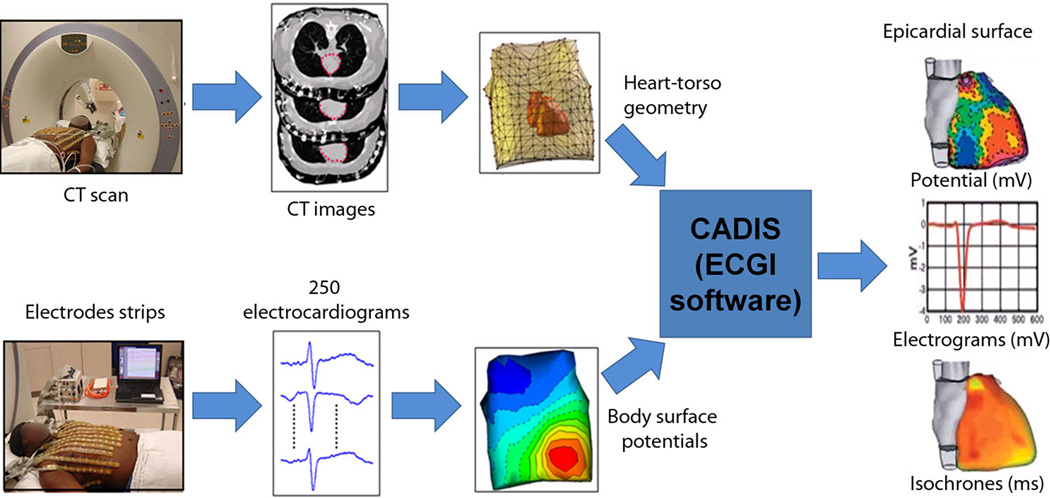
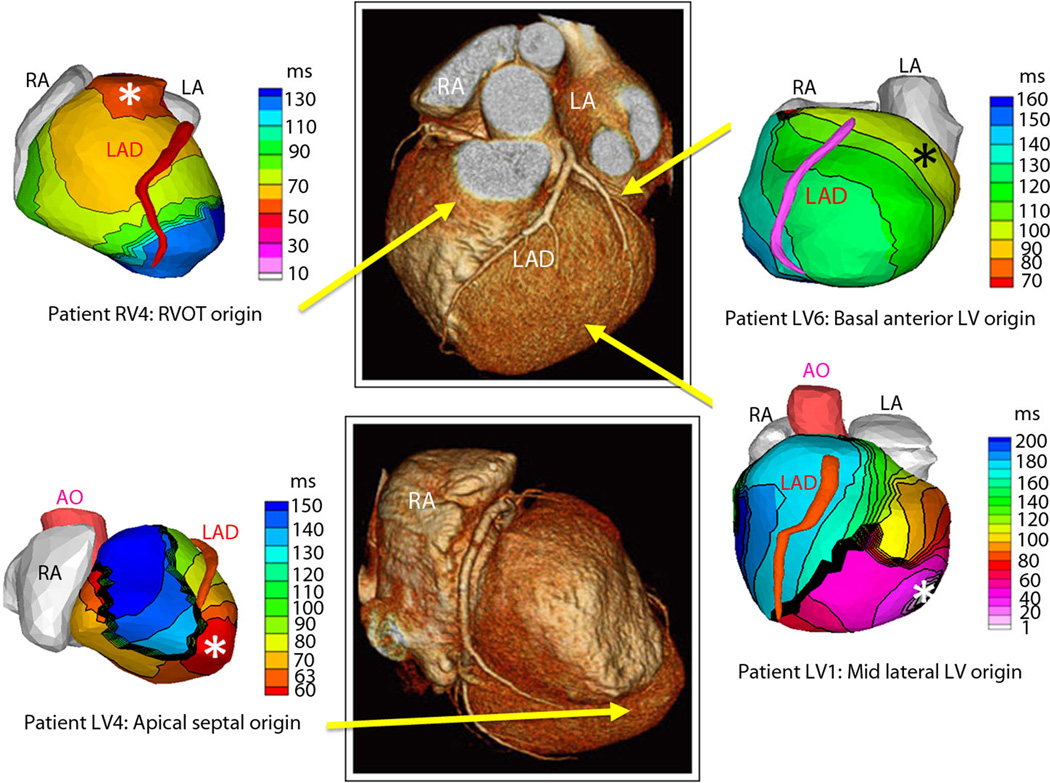
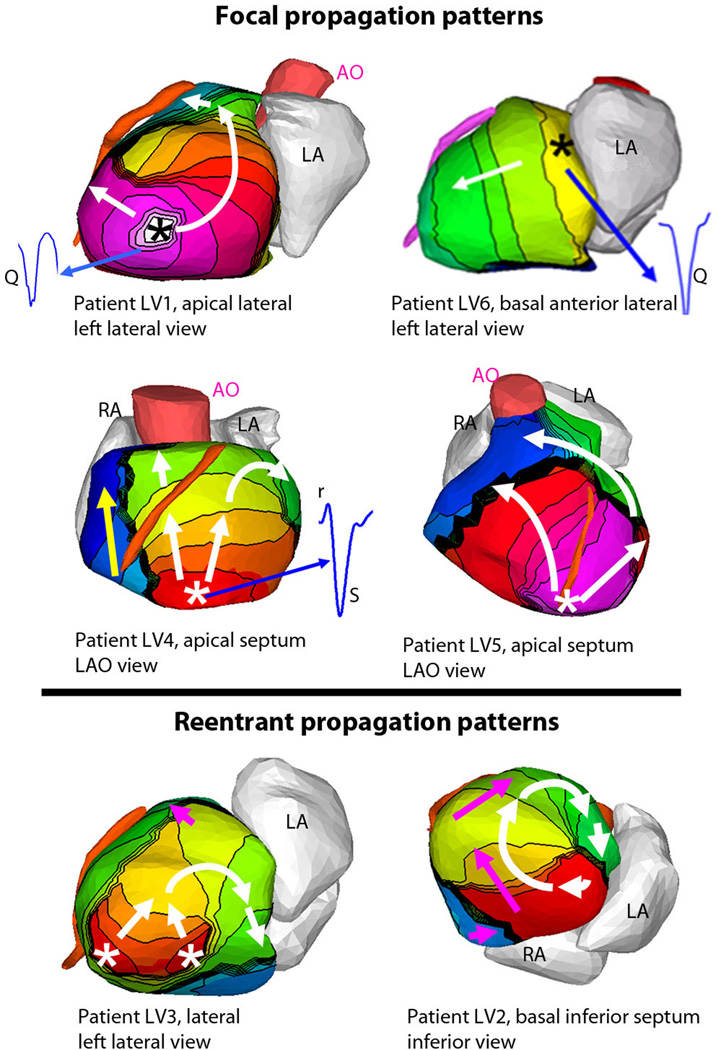
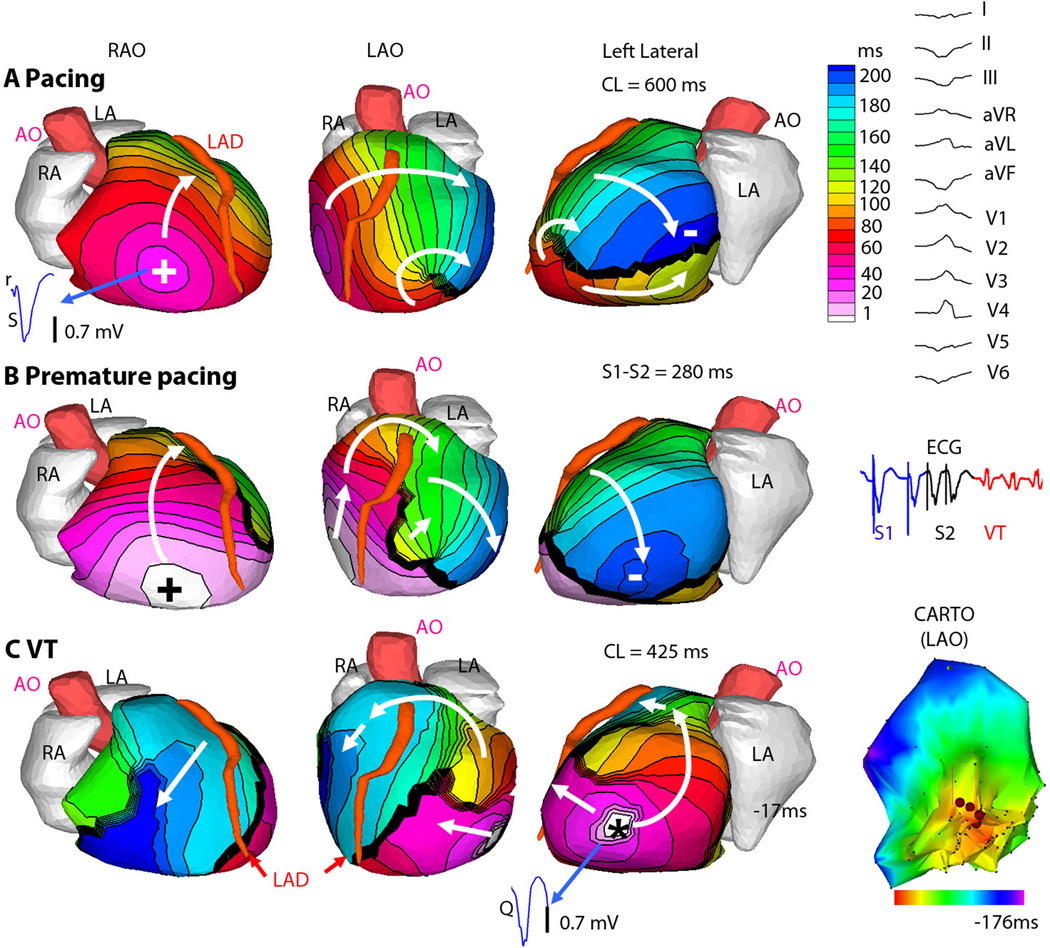
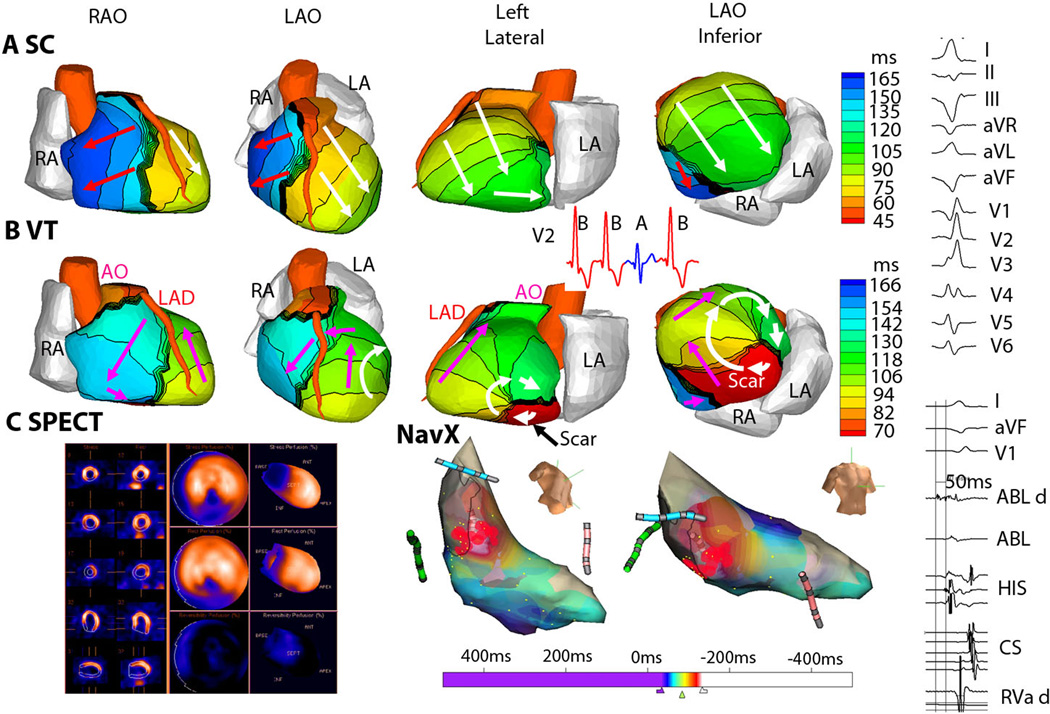
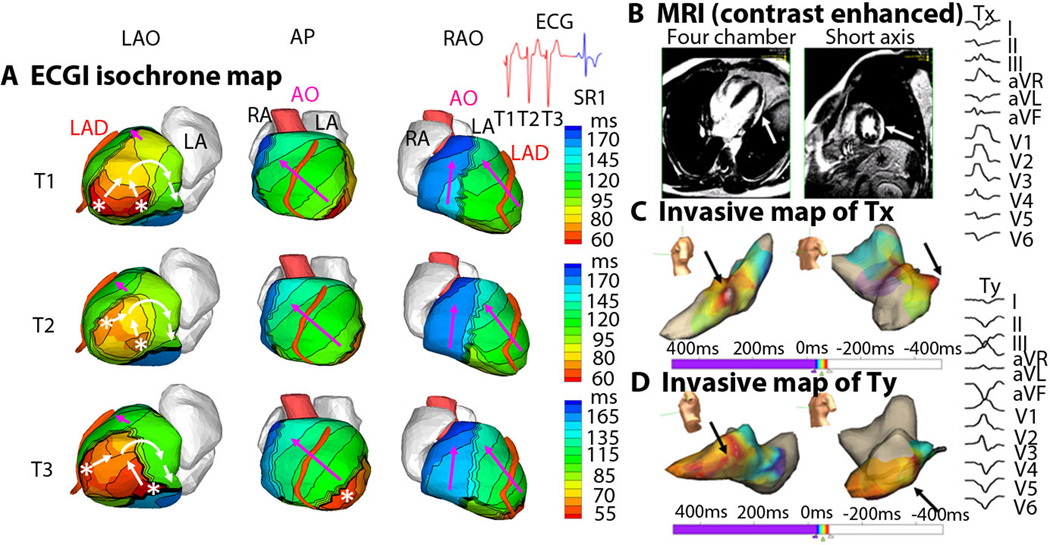
The rapid heartbeat of ventricular tachycardia (VT) can lead to sudden cardiac death and is a major health issue worldwide. Efforts to identify patients at risk, determine mechanisms of VT, and effectively prevent and treat VT through a mechanism-based approach would all be facilitated by continuous, noninvasive imaging of the arrhythmia over the entire heart. Here, we present noninvasive real-time images of human ventricular arrhythmias using electrocardiographic imaging (ECGI). Our results reveal diverse activation patterns, mechanisms, and sites of initiation of human VT. The spatial resolution of ECGI is superior to that of the routinely used 12-lead electrocardiogram, which provides only global information, and ECGI has distinct advantages over the currently used method of mapping with invasive catheter-applied electrodes. The spatial resolution of this method and its ability to image electrical activation sequences over the entire ventricular surfaces in a single heartbeat allowed us to determine VT initiation sites and continuation pathways, as well as VT relationships to ventricular substrates, including anatomical scars and abnormal electrophysiological substrate. Thus, ECGI can map the VT activation sequence and identify the location and depth of VT origin in individual patients, allowing personalized treatment of patients with ventricular arrhythmias.
Figures
Comment in
-
Imaging cardiac arrhythmias.Sci Transl Med. 2011 Aug 31;3(98):98fs2. doi: 10.1126/scitranslmed.3002806. Sci Transl Med. 2011. PMID: 21885402 Free PMC article.
References
-
- Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N. Engl. J. Med. 1996;335:1933–1940. - PubMed
-
- A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N. Engl. J. Med. 1997;337:1576–1583. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N. Engl. J. Med. 1999;341:1882–1890. - PubMed
-
- Wittig JH, Boineau JP. Surgical treatment of ventricular arrhythmia using epicardial, transmural, and endocardial mapping. Ann Thrac Surg. 1975;20:117–126. - PubMed
-
- Guiraudon G, Fontaine G, Frank R, Escande G, Etievent P, Cabrol C. Encircling endocardial ventriculotomy: a new surgical treatment for life-threatening ventricular tachycardias resistant to medical treatment following myocardial infarction. Ann Thorac Surg. 1978;26:438–444. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
