

Effect of manual lymph drainage in addition to guidelines and exercise therapy on arm lymphoedema related to breast cancer: randomised controlled trial
- PMID: 21885537
- PMCID: PMC3164214
- DOI: 10.1136/bmj.d5326
Effect of manual lymph drainage in addition to guidelines and exercise therapy on arm lymphoedema related to breast cancer: randomised controlled trial
Abstract
Objective: To determine the preventive effect of manual lymph drainage on the development of lymphoedema related to breast cancer.
Design: Randomised single blinded controlled trial.
Setting: University Hospitals Leuven, Leuven, Belgium.
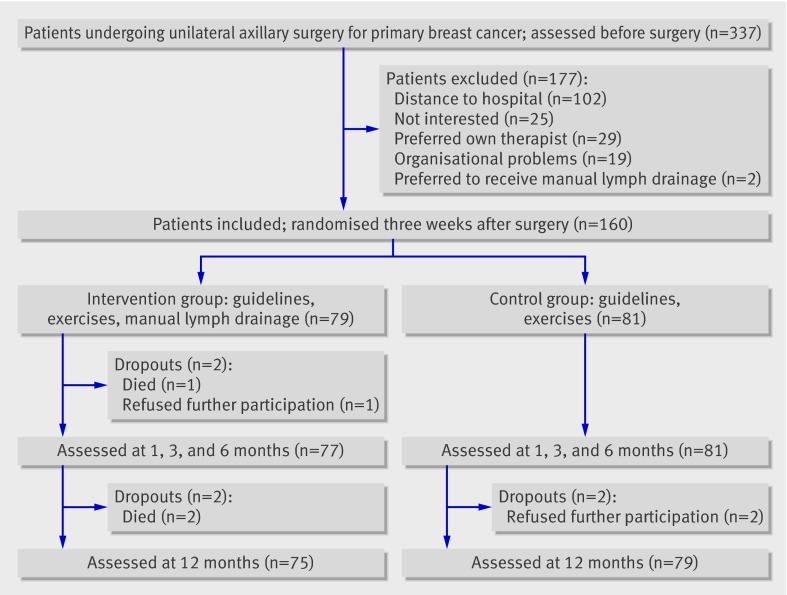
Participants: 160 consecutive patients with breast cancer and unilateral axillary lymph node dissection. The randomisation was stratified for body mass index (BMI) and axillary irradiation and treatment allocation was concealed. Randomisation was done independently from recruitment and treatment. Baseline characteristics were comparable between the groups.
Intervention: For six months the intervention group (n = 79) performed a treatment programme consisting of guidelines about the prevention of lymphoedema, exercise therapy, and manual lymph drainage. The control group (n = 81) performed the same programme without manual lymph drainage.
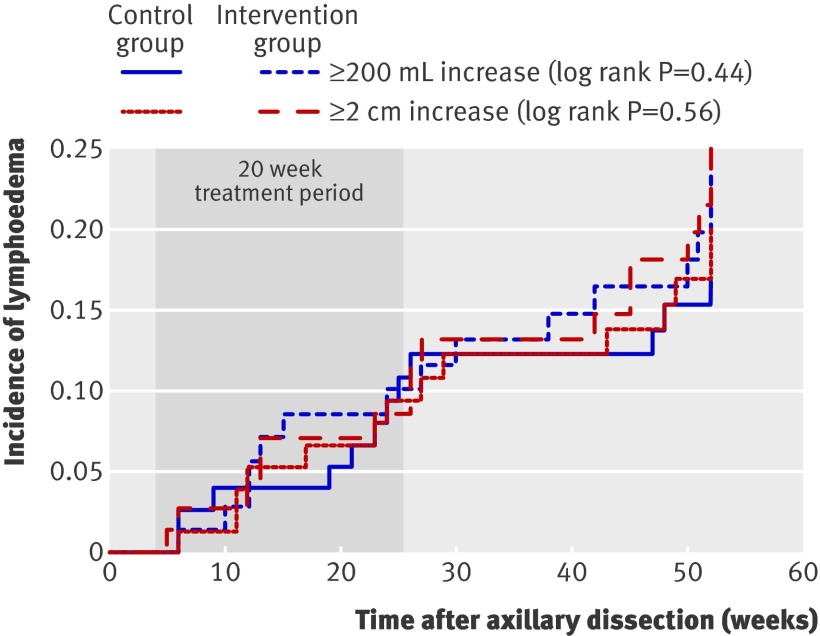
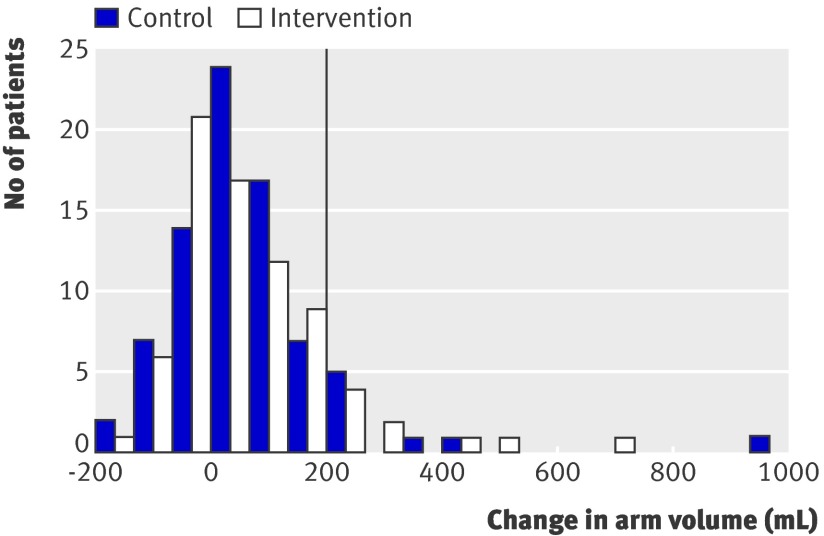
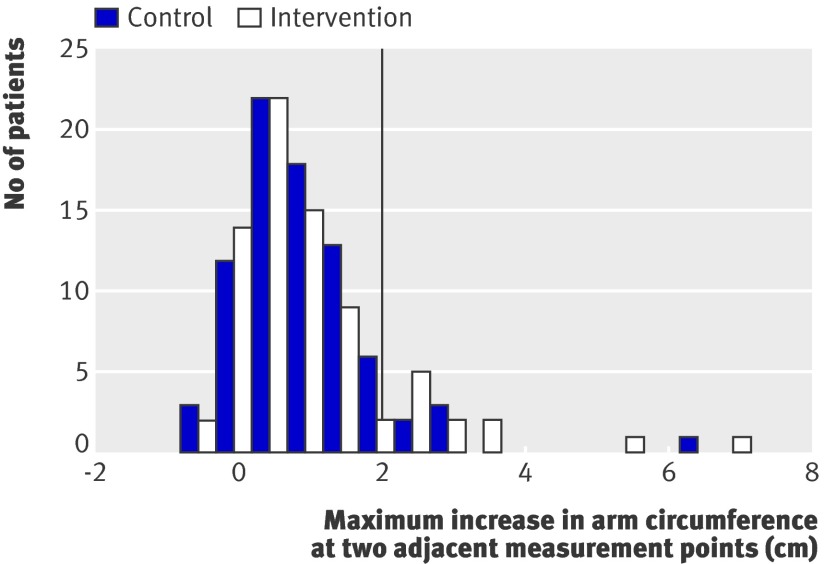
Main outcome measures: Cumulative incidence of arm lymphoedema and time to develop arm lymphoedema, defined as an increase in arm volume of 200 mL or more in the value before surgery.
Results: Four patients in the intervention group and two in the control group were lost to follow-up. At 12 months after surgery, the cumulative incidence rate for arm lymphoedema was comparable between the intervention group (24%) and control group (19%) (odds ratio 1.3, 95% confidence interval 0.6 to 2.9; P = 0.45). The time to develop arm lymphoedema was comparable between the two group during the first year after surgery (hazard ratio 1.3, 0.6 to 2.5; P = 0.49). The sample size calculation was based on a presumed odds ratio of 0.3, which is not included in the 95% confidence interval. This odds ratio was calculated as (presumed cumulative incidence of lymphoedema in intervention group/presumed cumulative incidence of no lymphoedema in intervention group)×(presumed cumulative incidence of no lymphoedema in control group/presumed cumulative incidence of lymphoedema in control group) or (10/90)×(70/30).
Conclusion: Manual lymph drainage in addition to guidelines and exercise therapy after axillary lymph node dissection for breast cancer is unlikely to have a medium to large effect in reducing the incidence of arm lymphoedema in the short term. Trial registration Netherlands Trial Register No NTR 1055.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Manual lymph drainage when added to advice and exercise may not be effective in preventing lymphoedema after surgery for breast cancer.J Physiother. 2011;57(4):258. doi: 10.1016/S1836-9553(11)70059-5. J Physiother. 2011. PMID: 22093127
References
-
- Berry DA, Cronin KA, Plevritis SK, Fryback DG, Clarke L, Zelen M, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med 2005;353:1784-92. - PubMed
-
- Foldi E, Foldi M, Clodius L. The lymphedema chaos: a lancet. Ann Plast Surg 1989;22:505-15. - PubMed
-
- Stanton AW, Modi S, Mellor RH, Levick JR, Mortimer PS. Recent advances in breast cancer-related lymphedema of the arm: lymphatic pump failure and predisposing factors. Lymphat Res Biol 2009;7:29-45. - PubMed
-
- Fleissig A, Fallowfield LJ, Langridge CI, Johnson L, Newcombe RG, Dixon JM, et al. Post-operative arm morbidity and quality of life. Results of the ALMANAC randomised trial comparing sentinel node biopsy with standard axillary treatment in the management of patients with early breast cancer. Breast Cancer Res Treat 2006;95:279-93. - PubMed
-
- Karki A, Simonen R, Malkia E, Selfe J. Impairments, activity limitations and participation restrictions 6 and 12 months after breast cancer operation. J Rehabil Med 2005;37:180-8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical