

Short- and intermediate-term angiographic and clinical outcomes of patients with various grades of coil protrusions following embolization of intracranial aneurysms
- PMID: 21885722
- PMCID: PMC7964362
- DOI: 10.3174/ajnr.A2572
Short- and intermediate-term angiographic and clinical outcomes of patients with various grades of coil protrusions following embolization of intracranial aneurysms
Abstract
Background and purpose: An infrequent occurrence during endovascular treatment is protusion of detachable coils into the parent lumen with a subsequent thrombosis within in the parent vessel or embolic events. We report the short- and intermediate-term angiographic and clinical outcomes of patients who experience coil or loop protrusions and are managed with medical or additional endovascular treatments.
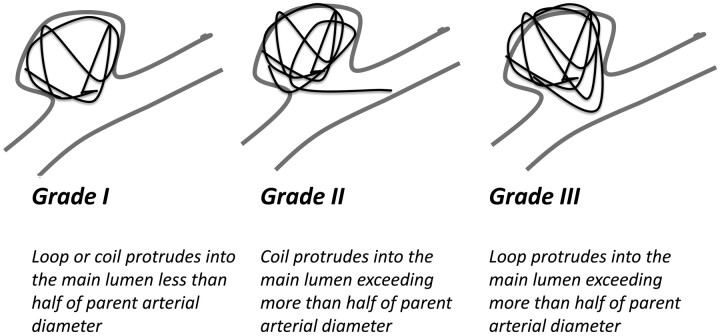
Materials and methods: The coil protrusions were identified by retrospective review of 256 consecutive patients treated at 3 centers with endovascular embolizations for intracranial aneurysms and subsequently categorized as grade I when a single loop or coil protruded into the parent vessel lumen less than half the parent artery diameter; grades II and III were assigned when a single coil or loop protruded more than half the parent artery diameter, respectively.
Results: There were 19 patients with grade I (n = 9), grade II (n = 4), or grade III (n = 6) coil protrusions. Patients with active hemodynamic compromise (n = 6) had intracranial stents placed in addition to aspirin (indefinitely) and clopidogrel (range, 1-12 months; mean, 4.5 months) treatment. The remaining patients were placed on aspirin indefinitely. Complete aneurysm obliteration was achieved in all patients except in 3 in whom near-complete obliteration was achieved. Two patients had intraprocedural aneurysm ruptures, both of whom survived hospitalization. There were 4 deaths (4-21 days), all due to major strokes in different vascular distributions related to vasospasm (unrelated to the coil protrusion).
Conclusions: Management of coil protrusions with antiplatelet therapy and placement of stents (in selected patients) appears efficacious in preventing vessel thrombosis.
Figures
Similar articles
-
Coil embolization for intracranial aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(1):1-114. Epub 2006 Jan 1. Ont Health Technol Assess Ser. 2006. PMID: 23074479 Free PMC article.
-
Complication analysis of intracranial aneurysm embolization with controllable coils.Chin Med Sci J. 2004 Mar;19(1):51-5. Chin Med Sci J. 2004. PMID: 15104225
-
Endovascular coil embolization of ruptured and unruptured posterior circulation aneurysms: review of a 10-year experience.Neurosurgery. 2007 Apr;60(4):626-36; discussion 636-7. doi: 10.1227/01.NEU.0000255433.47044.8F. Neurosurgery. 2007. PMID: 17415199
-
Complex intracranial aneurysms: combined operative and endovascular approaches.Neurosurgery. 1998 Dec;43(6):1304-12; discussion 1312-3. doi: 10.1097/00006123-199812000-00020. Neurosurgery. 1998. PMID: 9848843 Review.
-
Endovascular treatment of intracranial aneurysms with Guglielmi Detachable Coils: emphasis on new techniques.J Clin Neurosci. 2000 May;7(3):244-53. doi: 10.1054/jocn.1999.0211. J Clin Neurosci. 2000. PMID: 10833624 Review.
Cited by
-
Application of the Neuroform Atlas Stent in Intracranial Aneurysms: Current Status.Front Neurol. 2022 Mar 25;13:829143. doi: 10.3389/fneur.2022.829143. eCollection 2022. Front Neurol. 2022. PMID: 35401410 Free PMC article. Review.
-
Endovascular treatment of small (< 5 mm) unruptured middle cerebral artery aneurysms.Pol J Radiol. 2019 Apr 15;84:e198-e204. doi: 10.5114/pjr.2019.84829. eCollection 2019. Pol J Radiol. 2019. PMID: 31481991 Free PMC article.
-
Virtual coil images can optimize the visualization of the neckline of intracranial aneurysms during coil embolization: A technical note.Surg Neurol Int. 2023 Sep 29;14:349. doi: 10.25259/SNI_675_2023. eCollection 2023. Surg Neurol Int. 2023. PMID: 37810302 Free PMC article.
-
Surgical recanalization of distal middle cerebral artery occlusion due to a coil migration during endovascular coil embolization: a case report.J Cerebrovasc Endovasc Neurosurg. 2014 Sep;16(3):287-92. doi: 10.7461/jcen.2014.16.3.287. Epub 2014 Sep 30. J Cerebrovasc Endovasc Neurosurg. 2014. PMID: 25340033 Free PMC article.
-
Stent-Assisted Clip Placement for Complex Internal Carotid Artery Intracranial Aneurysms.J Vasc Interv Neurol. 2016 Jan;8(5):23-9. J Vasc Interv Neurol. 2016. PMID: 26958150 Free PMC article.
References
-
- Vanninen R, Koivisto T, Saari T, et al. . Ruptured intracranial aneurysms: acute endovascular treatment with electrolytically detachable coils—a prospective randomized study. Radiology 1999; 211: 325– 36 - PubMed
-
- Dinc H, Kuzeyli K, Kosucu P, et al. . Retrieval of prolapsed coils during endovascular treatment of cerebral aneurysms. Neuroradiology 2006; 48: 269– 72 - PubMed
-
- Fessler R, Ringer A, Qureshi A, et al. . Intracranial stent placement to trap an extruded coil during endovascular aneurysm treatment: technical note. Neurosurgery 2000; 46: 248– 53, discussion 251–53 - PubMed
-
- Lanzino G, Wakhloo A, Fessler R, et al. . Efficacy and current limitations of intravascular stents for intracranial internal carotid, vertebral, basilar artery aneurysms. J Neurosurg 1999; 91: 538– 46 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical