

The use of the Oxford classification of IgA nephropathy to predict renal survival
- PMID: 21885791
- PMCID: PMC3359557
- DOI: 10.2215/CJN.01170211
The use of the Oxford classification of IgA nephropathy to predict renal survival
Abstract
Background and objectives: A new classification for IgA nephropathy was recently proposed, namely the Oxford classification. It established specific pathologic features that predict the risk of progression of renal disease. This classification needs validation in different patient populations. We propose a retrospective study to evaluate the predictive value of the Oxford classification on renal survival defined by doubling creatinine or end-stage renal disease in patients with IgA nephropathy.
Design, setting, participants, & measurements: We included 183 patients with primary IgA nephropathy diagnosed between 1994 and 2005. Mean follow-up time was 77 months. Doubling creatinine occurred in 20% of the patients, and end-stage renal disease occurred in 16%. The biopsies were revisited to apply the Oxford classification. The influence of pathologic features on renal survival was analyzed in univariate and multivariate models.
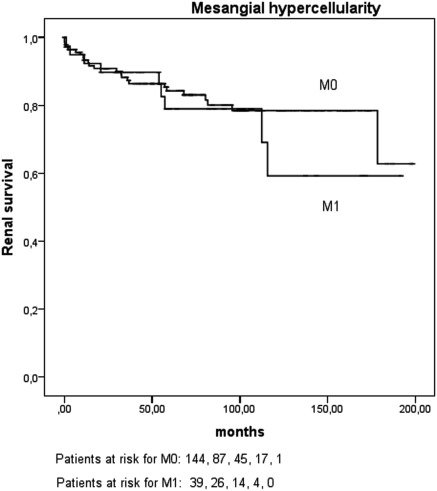
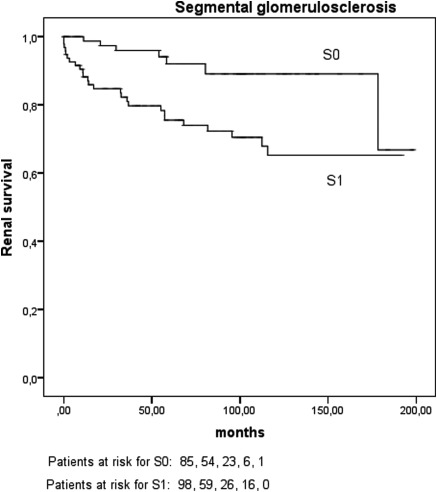
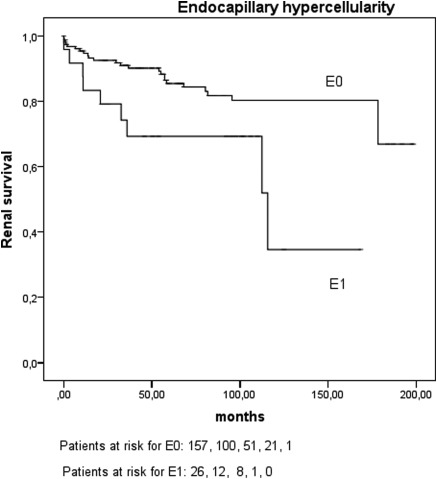
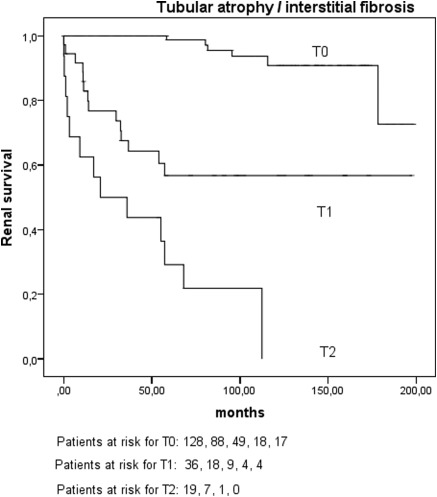
Results: In univariate time-dependent analyses, tubular atrophy/interstitial fibrosis, segmental glomerulosclerosis, and endocapillary hypercellularity strongly impacted doubling creatinine or end-stage renal disease. On the contrary, mesangial hypercellularity was not associated with renal outcome. In the multivariate model, only estimated GFR at baseline was a risk factor, pathologic lesions having no independent influence.
Conclusions: We confirm the usefulness of the Oxford classification to establish the renal prognosis of patients with IgA nephropathy, although renal function at baseline seems to be of a greater importance than pathologic lesions.
Figures
Comment in
-
Validating the oxford classification of IgA nephropathy.Clin J Am Soc Nephrol. 2011 Oct;6(10):2335-6. doi: 10.2215/CJN.08440811. Clin J Am Soc Nephrol. 2011. PMID: 21979911 No abstract available.
References
-
- D'Amico G: Natural history of idiopathic IgA nephropathy: Role of clinical and histological prognostic factors. Am J Kidney Dis 36: 227–237, 2000 - PubMed
-
- Laville M, Alamartine E: Treatment options for IgA nephropathy in adults: A proposal for evidence-based strategy. Nephrol Dial Transplant 19: 1947–1951, 2004 - PubMed
-
- Alamartine E, Sabatier JC, Berthoux FC: Comparison of pathological lesions on repeated renal biopsies in 73 patients with primary IgA glomerulonephritis: Value of quantitative scoring and approach to final prognosis. Clin Nephrol 34: 45–51, 1990 - PubMed
-
- Radford MG, Jr, Donadio JV, Jr, Bergstralh EJ, Grande JP: Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol 8: 199–207, 1997 - PubMed
-
- Katafuchi R, Kiyoshi Y, Oh Y, Uesugi N, Ikeda K, Yanase T, Fujimi S: Glomerular score as a prognosticator in IgA nephropathy: Its usefulness and limitation. Clin Nephrol 49: 1–8, 1998 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
