

Tuberculosis in indigenous peoples in the U.S., 2003-2008
- PMID: 21886328
- PMCID: PMC3151185
- DOI: 10.1177/003335491112600510
Tuberculosis in indigenous peoples in the U.S., 2003-2008
Abstract
Objectives: We examined trends and epidemiology of tuberculosis (TB) across racial/ethnic groups to better understand TB disparities in the United States, with particular focus on American Indians/Alaska Natives (AI/ANs) and Native Hawaiians/other Pacific Islanders (NH/PIs).
Methods: We analyzed cases in the U.S. National Tuberculosis Surveillance System and calculated TB case rates among all racial/ethnic groups from 2003 to 2008. Socioeconomic and health indicators for counties in which TB cases were reported came from the Health Resources and Services Administration Area Resource File.
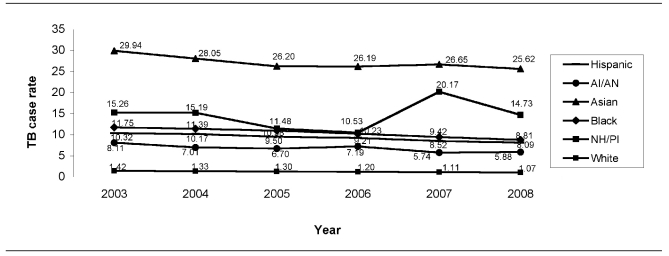
Results: Among the 82,836 TB cases, 914 (1.1%) were in AI/ANs and 362 (0.4%) were in NH/PIs. In 2008, TB case rates for AI/ANs and NH/PIs were 5.9 and 14.7 per 100,000 population, respectively, rates that were more than five and 13 times greater than for non-Hispanic white people (1.1 per 100,000 population). From 2003 to 2008, AI/ANs had the largest percentage decline in TB case rates (-27.4%) for any racial/ethnic group, but NH/PIs had the smallest percentage decline (-3.5%). AI/ANs were more likely than other racial/ethnic groups to be homeless, excessively use alcohol, receive totally directly observed therapy, and come from counties with a greater proportion of people living in poverty and without health insurance. A greater proportion of NH/PIs had extrapulmonary disease and came from counties with a higher proportion of people with a high school diploma.
Conclusions: There is a need to develop flexible TB-control strategies that address the social determinants of health and that are tailored to the specific needs of AI/ANs and NH/PIs in the U.S.
Figures
References
-
- World Health Organization. Global tuberculosis control 2009—- epidemiology, strategy, financing. Geneva: WHO; 2009.
-
- UN Permanent Forum on Indigenous Issues. State of the world's indigenous peoples. New York: United Nations; 2009. [cited 2011 Mar 29]. Also available from: URL: http://www.un.org/esa/socdev/unpfii/documents/SOWIP_web.pdf.
-
- Das D, Baker M, Calder L. Tuberculosis epidemiology in New Zealand: 1995–2004. N Z Med J. 2006;119:U2249. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
