

Radiographic and endoscopic diagnosis and treatment of enterocutaneous fistulas
- PMID: 21886464
- PMCID: PMC2967314
- DOI: 10.1055/s-0030-1262982
Radiographic and endoscopic diagnosis and treatment of enterocutaneous fistulas
Abstract
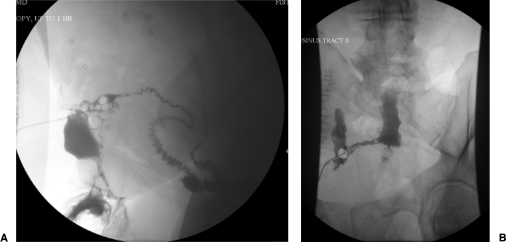
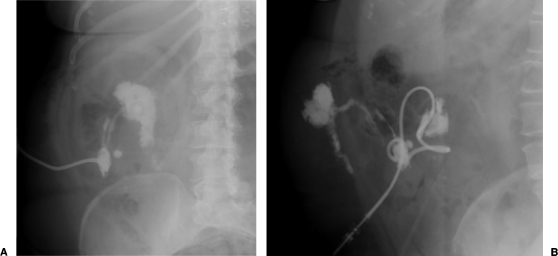
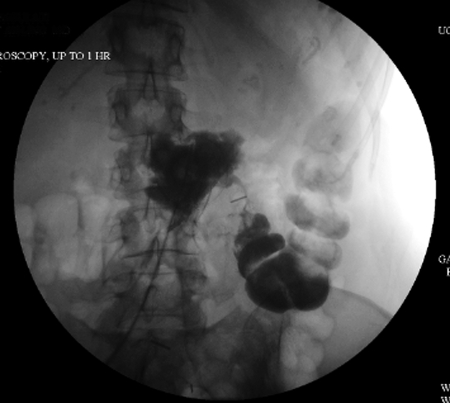
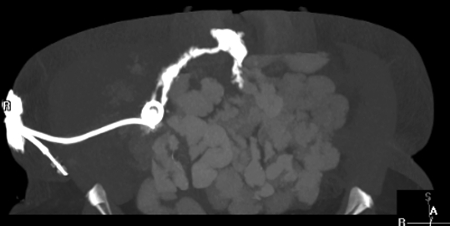
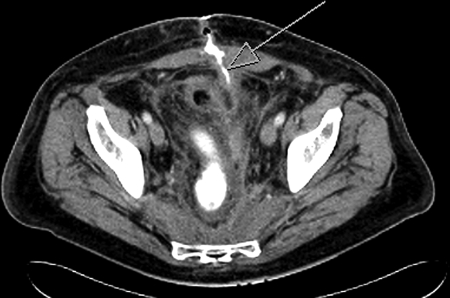
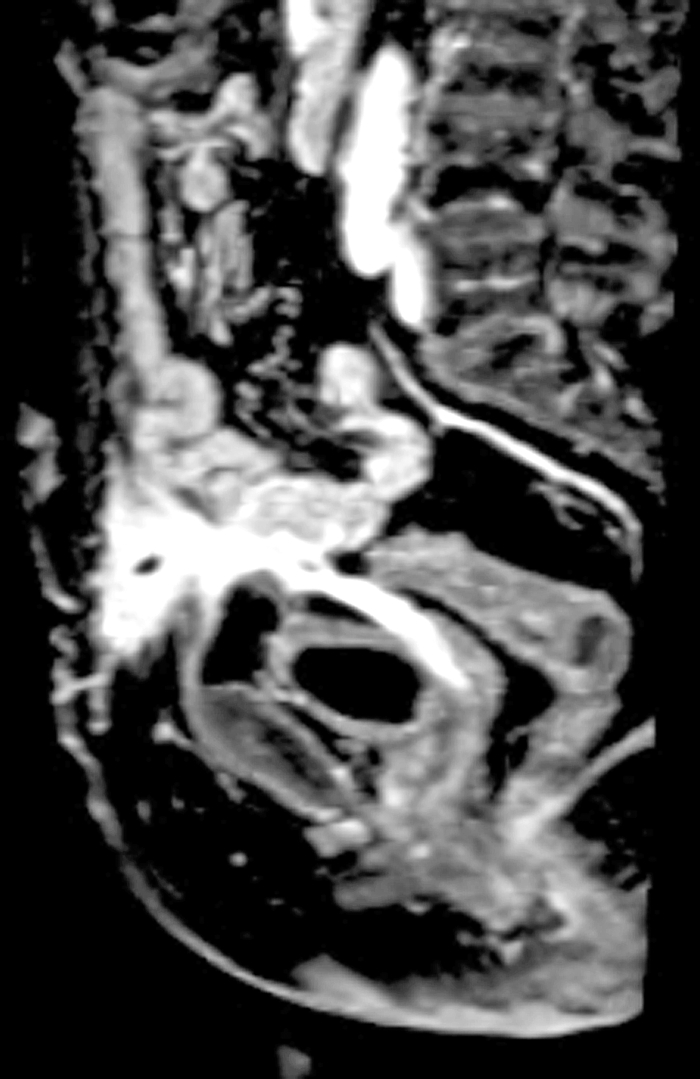
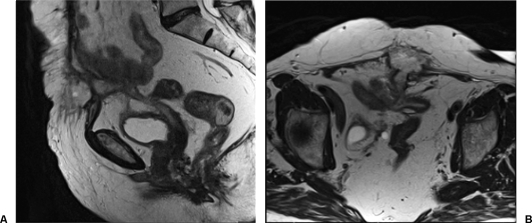
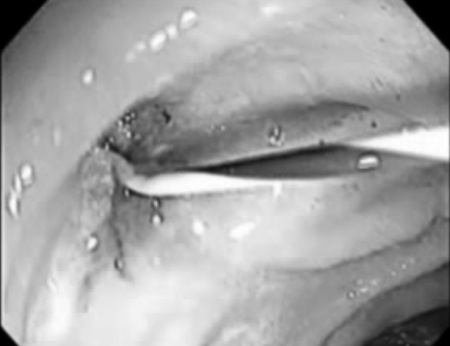
The management of enterocutaneous fistulas continues to be a challenging postoperative complication. Understanding the anatomy of the fistula optimizes its evaluation and management. Diagnostic radiology has always played an important role in this task. The use of plain radiography with contrasted studies and fistulograms is well documented in the earliest investigations of fistulas and they continue to be helpful techniques. The imaging techniques have evolved rapidly over the past 15 years with the introduction of cross-sectional imaging, ultrasound and endoscopy. The purpose of this chapter is to review both the diagnostic and therapeutic roles of fistulograms, small bowel follow-through, computed tomography, magnetic resonance imaging, ultrasound, and endoscopy in the setting of acquired enterocutaneous fistulas.
Keywords: Enterocutaneous fistula; computed tomography; fistulogram; magnetic resonance imaging; small bowel follow-through.
Figures




References
-
- Rankin F W, Bargen J A, Buie L A. The Colon, Rectum, and Anus. Philadelphia: Saunders; 1932. p. 346.
-
- Lewis D, Penick R M. Fecal fistula. Internat Clin. 1933;1:111.
-
- Ransom H K, Coller F A. Intestinal fistula. J Mich State Med S. 1935;34:281.
LinkOut - more resources
Full Text Sources
Miscellaneous
