

Traumatic osteochondral injury of the femoral head treated by mosaicplasty: a report of two cases
- PMID: 21886541
- PMCID: PMC2926357
- DOI: 10.1007/s11420-010-9159-y
Traumatic osteochondral injury of the femoral head treated by mosaicplasty: a report of two cases
Abstract
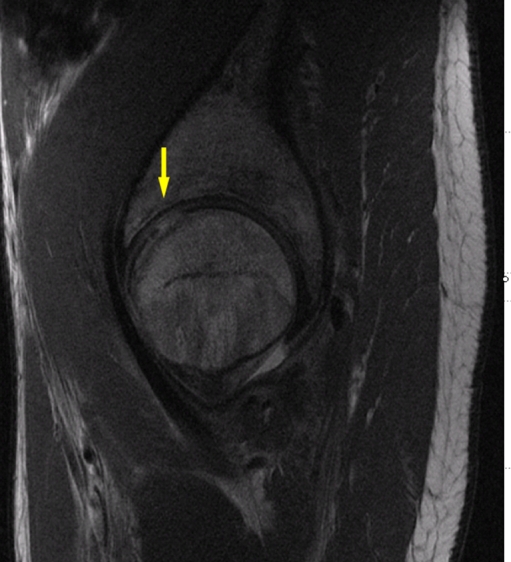
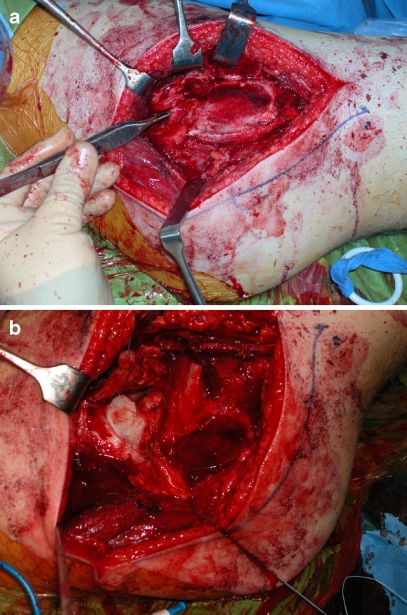
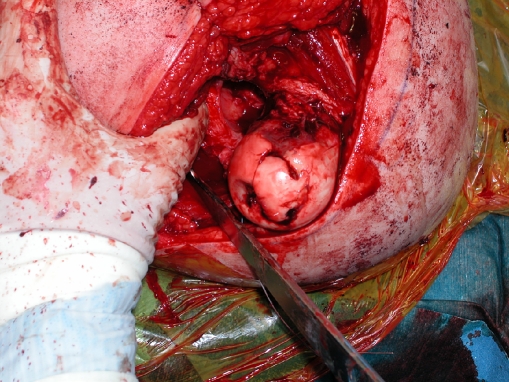
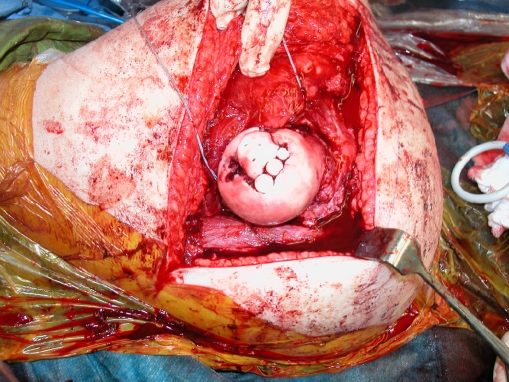
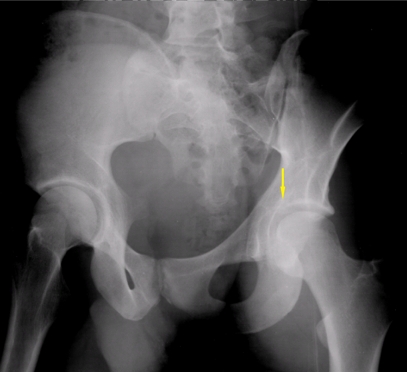
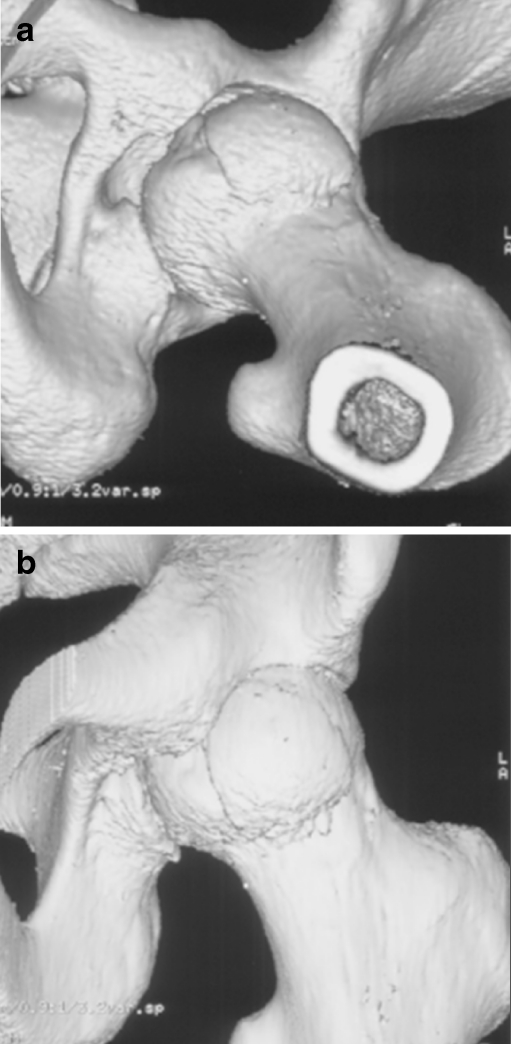
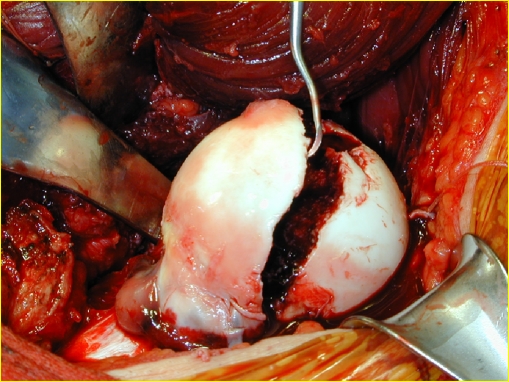
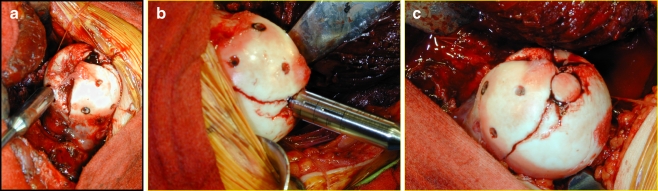
The increased risk of symptomatic progression towards osteoarthritis after chondral damage has led to the development of multiple treatment options for cartilage repair. These procedures have evolved from arthroscopic lavage and debridement, to marrow stimulation techniques, and more recently, to osteochondral autograft and allograft transplants, and autogenous chondrocyte implantation. The success of mosaicplasty procedures in the knee has led to its application to other surfaces, including the talus, tibial plateau, patella, and humeral capitellum. In this report, we present two cases of a chondral defect to the femoral head after a traumatic hip dislocation, treated with an osteochondral autograft (OATS) from the ipsilateral knee, and the inferior femoral head, respectively, combined with a surgical dislocation of the hip. At greater than 1 year and greater than 5 years of follow-up, MRI studies have demonstrated good autograft incorporation with maintenance of articular surface conformity, and both patients clinically continue to have no pain and full active range of motion of their respective hips. In our opinion, treatment of osteochondral defects in the femoral head surface using a surgical dislocation combined with an OATS procedure is a promising approach, as full exposure of the femoral head can be obtained while preserving its vasculature, thus enabling adequate restoration of the articular cartilage surface.
Keywords: femoral head; hip dislocation; mosaicplasty; osteochondral autograft transplant; osteochondral defect; osteochondral injury.
Figures





References
-
- Steadman JR, Rodkey WG, Briggs KK. Microfracture to treat full-thickness chondral defects: Surgical technique, rehabilitation, and outcomes. J Knee Surg. 2002;15:170–176. - PubMed
-
- Buckwalter JA, Mow VC, Ratcliffe A. Restoration of injured or degenerated articular cartilage. J Am Acad Orthop Surg. 1994;2:192–201. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
