

Mobilisation of hematopoietic CD34+ precursor cells in patients with acute stroke is safe--results of an open-labeled non randomized phase I/II trial
- PMID: 21887230
- PMCID: PMC3162562
- DOI: 10.1371/journal.pone.0023099
Mobilisation of hematopoietic CD34+ precursor cells in patients with acute stroke is safe--results of an open-labeled non randomized phase I/II trial
Abstract
Background: Regenerative strategies in the treatment of acute stroke may have great potential. Hematopoietic growth factors mobilize hematopoietic stem cells and may convey neuroprotective effects. We examined the safety, potential functional and structural changes, and CD34(+) cell-mobilization characteristics of G-CSF treatment in patients with acute ischemic stroke.
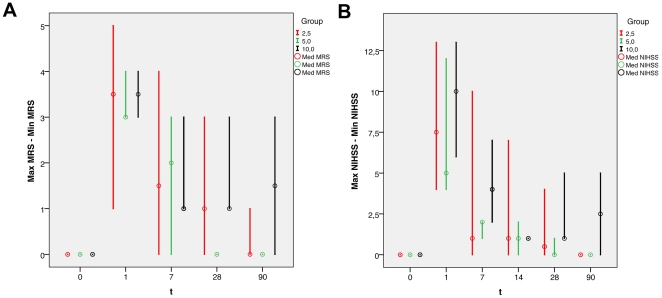
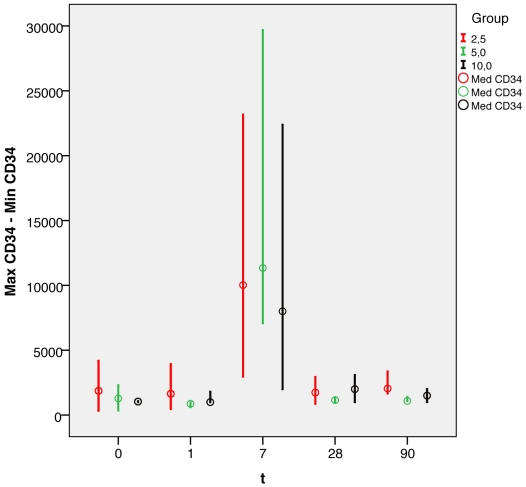
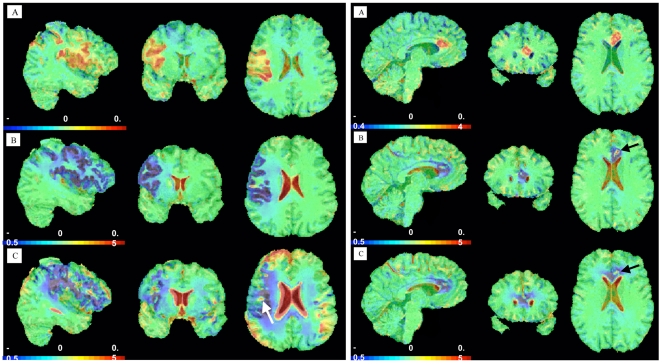
Methods and results: Three cohorts of patients (8, 6, and 6 patients per cohort) were treated subcutaneously with 2.5, 5, or 10 µg/kg body weight rhG-CSF for 5 consecutive days within 12 hrs of onset of acute stroke. Standard treatment included i.v. thrombolysis. Safety monitoring consisted of obtaining standardized clinical assessment scores, monitoring of CD34(+) stem cells, blood chemistry, serial neuroradiology, and neuropsychology. Voxel-guided morphometry (VGM) enabled an assessment of changes in the patients' structural parenchyma. 20 patients (mean age 55 yrs) were enrolled in this study, 5 of whom received routine thrombolytic therapy with r-tPA. G-CSF treatment was discontinued in 4 patients because of unrelated adverse events. Mobilization of CD34(+) cells was observed with no concomitant changes in blood chemistry, except for an increase in the leukocyte count up to 75,500/µl. Neuroradiological and neuropsychological follow-up studies did not disclose any specific G-CSF toxicity. VGM findings indicated substantial atrophy of related hemispheres, a substantial increase in the CSF space, and a localized increase in parenchyma within the ischemic area in 2 patients.
Conclusions: We demonstrate a good safety profile for daily administration of G-CSF when begun within 12 hours after onset of ischemic stroke and, in part in combination with routine i.v. thrombolysis. Additional analyses using VGM and a battery of neuropsychological tests indicated a positive functional and potentially structural effect of G-CSF treatment in some of our patients.
Trial registration: German Clinical Trial Register DRKS 00000723.
Conflict of interest statement
Figures
References
-
- Heart Disease and Stroke Statistics - 2006 Update. Dallas: American Heart Association; - PubMed
-
- Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, et al. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 jto 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. Jama. 1999;282:2019–2026. - PubMed
-
- Albers GW, Olivot JM. Intravenous alteplase for ischaemic stroke. Lancet. 2007;369:249–250. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Alberts MJ, Brass LM, Perry A, Webb D, Dawson DV. Evaluation times for patients with in-hospital strokes. Stroke. 1993;24:1817–1822. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
