

Albiglutide, a long lasting glucagon-like peptide-1 analog, protects the rat heart against ischemia/reperfusion injury: evidence for improving cardiac metabolic efficiency
- PMID: 21887274
- PMCID: PMC3162574
- DOI: 10.1371/journal.pone.0023570
Albiglutide, a long lasting glucagon-like peptide-1 analog, protects the rat heart against ischemia/reperfusion injury: evidence for improving cardiac metabolic efficiency
Abstract
Background: The cardioprotective effects of glucagon-like peptide-1 (GLP-1) and analogs have been previously reported. We tested the hypothesis that albiglutide, a novel long half-life analog of GLP-1, may protect the heart against I/R injury by increasing carbohydrate utilization and improving cardiac energetic efficiency.
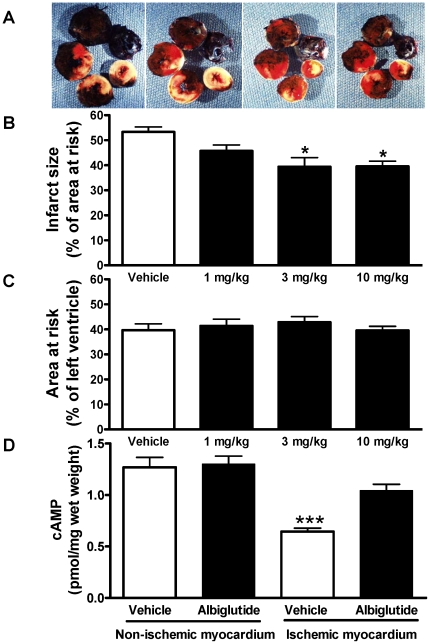
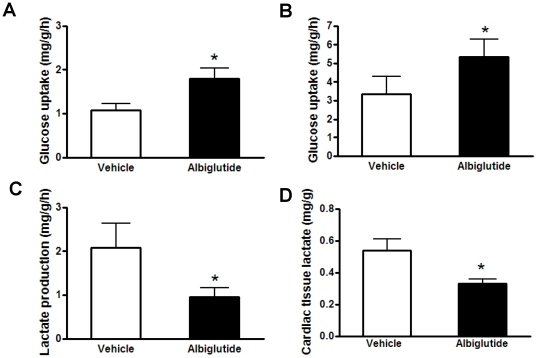
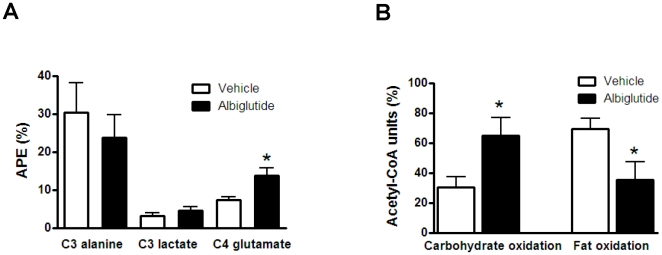
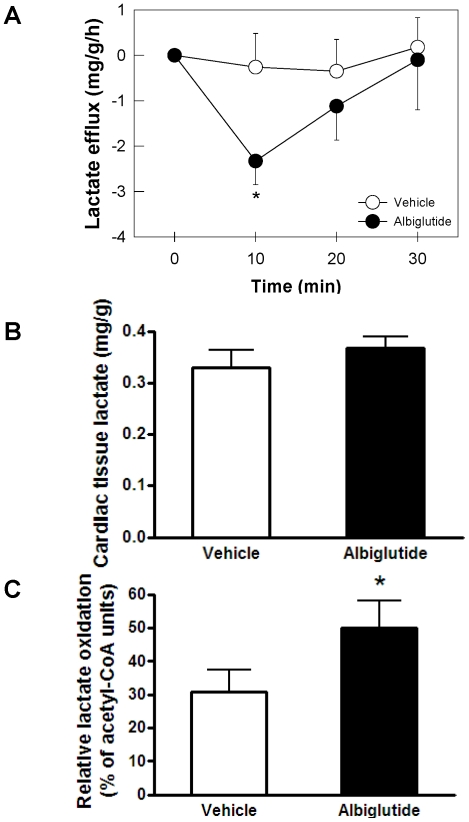
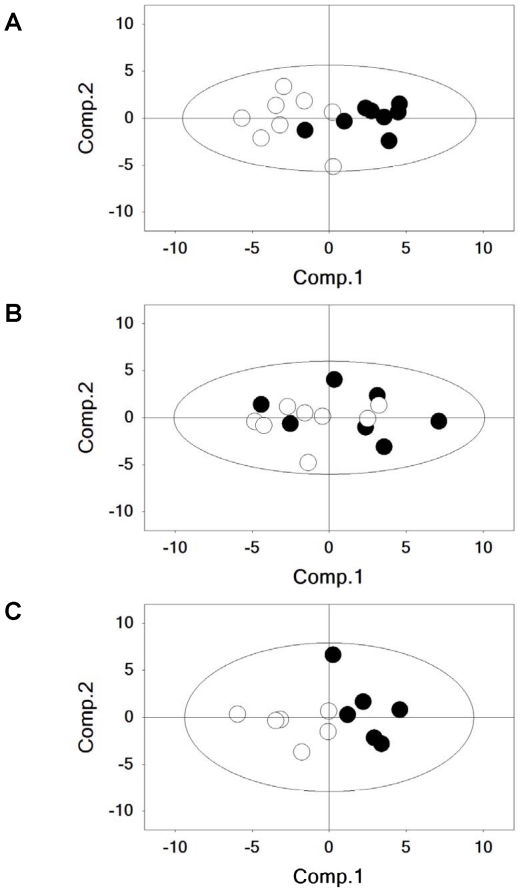
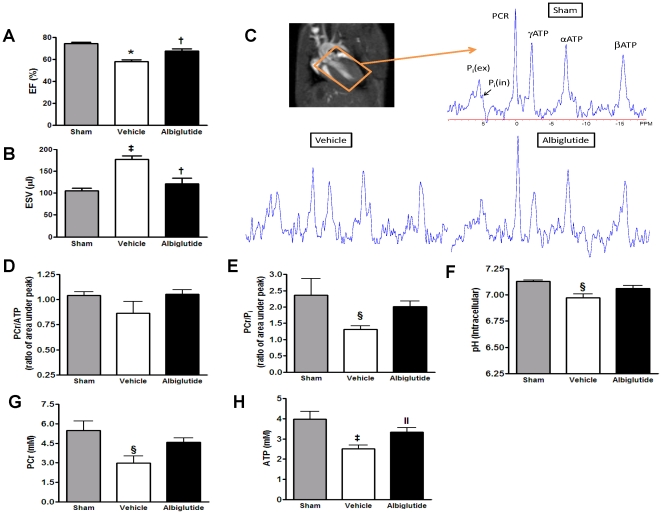
Methods/principal findings: Sprague-Dawley rats were treated with albiglutide and subjected to 30 min myocardial ischemia followed by 24 h reperfusion. Left ventricle infarct size, hemodynamics, function and energetics were determined. In addition, cardiac glucose disposal, carbohydrate metabolism and metabolic gene expression were assessed. Albiglutide significantly reduced infarct size and concomitantly improved post-ischemic hemodynamics, cardiac function and energetic parameters. Albiglutide markedly increased both in vivo and ex vivo cardiac glucose uptake while reducing lactate efflux. Analysis of metabolic substrate utilization directly in the heart showed that albiglutide increased the relative carbohydrate versus fat oxidation which in part was due to an increase in both glucose and lactate oxidation. Metabolic gene expression analysis indicated upregulation of key glucose metabolism genes in the non-ischemic myocardium by albiglutide.
Conclusion/significance: Albiglutide reduced myocardial infarct size and improved cardiac function and energetics following myocardial I/R injury. The observed benefits were associated with enhanced myocardial glucose uptake and a shift toward a more energetically favorable substrate metabolism by increasing both glucose and lactate oxidation. These findings suggest that albiglutide may have direct therapeutic potential for improving cardiac energetics and function.
Conflict of interest statement
Figures
Similar articles
-
Novel fusion of GLP-1 with a domain antibody to serum albumin prolongs protection against myocardial ischemia/reperfusion injury in the rat.Cardiovasc Diabetol. 2013 Oct 14;12:148. doi: 10.1186/1475-2840-12-148. Cardiovasc Diabetol. 2013. PMID: 24125539 Free PMC article.
-
Cardioprotection Resulting from Glucagon-Like Peptide-1 Administration Involves Shifting Metabolic Substrate Utilization to Increase Energy Efficiency in the Rat Heart.PLoS One. 2015 Jun 22;10(6):e0130894. doi: 10.1371/journal.pone.0130894. eCollection 2015. PLoS One. 2015. PMID: 26098939 Free PMC article.
-
Postconditioning with curaglutide, a novel GLP-1 analog, protects against heart ischemia-reperfusion injury in an isolated rat heart.Regul Pept. 2012 Oct 10;178(1-3):51-5. doi: 10.1016/j.regpep.2012.06.007. Epub 2012 Jun 29. Regul Pept. 2012. PMID: 22749991
-
Cardiac protection via metabolic modulation: an emerging role for incretin-based therapies?Cardiovasc Hematol Agents Med Chem. 2012 Dec;10(4):319-24. doi: 10.2174/187152512803530360. Cardiovasc Hematol Agents Med Chem. 2012. PMID: 22827290 Review.
-
Research progress on the effects of novel hypoglycemic drugs in diabetes combined with myocardial ischemia/reperfusion injury.Ageing Res Rev. 2023 Apr;86:101884. doi: 10.1016/j.arr.2023.101884. Epub 2023 Feb 16. Ageing Res Rev. 2023. PMID: 36801379 Review.
Cited by
-
Novel fusion of GLP-1 with a domain antibody to serum albumin prolongs protection against myocardial ischemia/reperfusion injury in the rat.Cardiovasc Diabetol. 2013 Oct 14;12:148. doi: 10.1186/1475-2840-12-148. Cardiovasc Diabetol. 2013. PMID: 24125539 Free PMC article.
-
PEGylated exendin-4, a modified GLP-1 analog exhibits more potent cardioprotection than its unmodified parent molecule on a dose to dose basis in a murine model of myocardial infarction.Theranostics. 2015 Jan 1;5(3):240-50. doi: 10.7150/thno.10226. eCollection 2015. Theranostics. 2015. PMID: 25553112 Free PMC article.
-
Glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1: Incretin actions beyond the pancreas.J Diabetes Investig. 2013 Mar 18;4(2):108-30. doi: 10.1111/jdi.12065. J Diabetes Investig. 2013. PMID: 24843641 Free PMC article. Review.
-
Cardioprotection Resulting from Glucagon-Like Peptide-1 Administration Involves Shifting Metabolic Substrate Utilization to Increase Energy Efficiency in the Rat Heart.PLoS One. 2015 Jun 22;10(6):e0130894. doi: 10.1371/journal.pone.0130894. eCollection 2015. PLoS One. 2015. PMID: 26098939 Free PMC article.
-
Systematic Understanding of Pathophysiological Mechanisms of Oxidative Stress-Related Conditions-Diabetes Mellitus, Cardiovascular Diseases, and Ischemia-Reperfusion Injury.Front Cardiovasc Med. 2021 Apr 13;8:649785. doi: 10.3389/fcvm.2021.649785. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33928135 Free PMC article. Review.
References
-
- Baggio LL, Drucker DJ. Biology of incretins GLP-1 and GIP. Gastroenterology. 2007;132:2131–2157. - PubMed
-
- Barnett AH. New treatments in type 2 diabetes: a focus on the incretin-based therapies. Clin Endocrinol (Oxf) 2009;70:343–353. - PubMed
-
- Bose AK, Mocanu MM, Carr RD, Yellon DM. Glucagon like peptide-1 is protective against myocardial ischemia/reperfusion injury when given either as a preconditioning mimetic or at reperfusion in an isolated rat heart model. Cardiovasc Drugs Ther. 2005;19:9–11. - PubMed
-
- Bose AK, Mocanu MM, Carr RD, Brand CL, Yellon DM. Glucagon-like peptide 1 can directly protect the heart against ischemia/reperfusion injury. Diabetes. 2005;54:146–151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
