

Clinical review: Special populations--critical illness and pregnancy
- PMID: 21888683
- PMCID: PMC3387584
- DOI: 10.1186/cc10256
Clinical review: Special populations--critical illness and pregnancy
Abstract
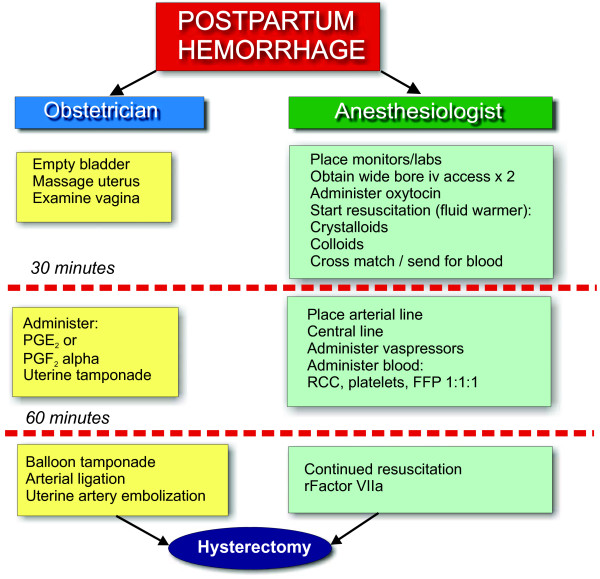
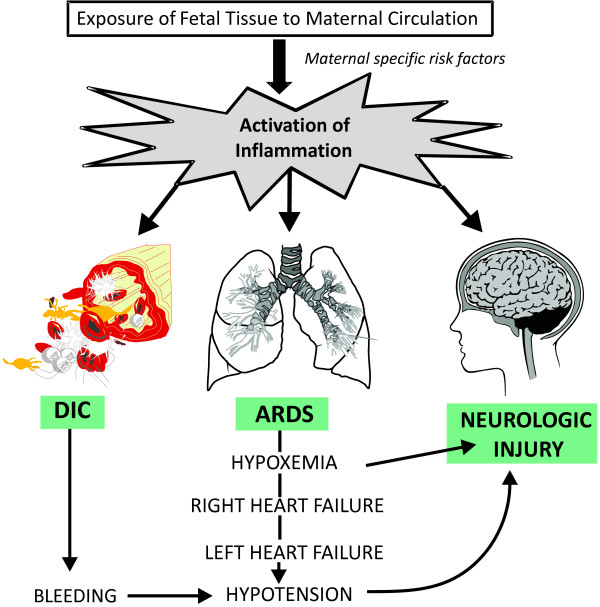
Critical illness is an uncommon but potentially devastating complication of pregnancy. The majority of pregnancy-related critical care admissions occur postpartum. Antenatally, the pregnant patient is more likely to be admitted with diseases non-specific to pregnancy, such as pneumonia. Pregnancy-specific diseases resulting in ICU admission include obstetric hemorrhage, pre-eclampsia/eclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, amniotic fluid embolus syndrome, acute fatty liver of pregnancy, and peripartum cardiomyopathy. Alternatively, critical illness may result from pregnancy-induced worsening of pre-existing diseases (for example, valvular heart disease, myasthenia gravis, and kidney disease). Pregnancy can also predispose women to diseases seen in the non-pregnant population, such as acute respiratory distress syndrome (for example, pneumonia and aspiration), sepsis (for example, chorioamnionitis and pyelonephritis) or pulmonary embolism. The pregnant patient may also develop conditions co-incidental to pregnancy such as trauma or appendicitis. Hemorrhage, particularly postpartum, and hypertensive disorders of pregnancy remain the most frequent indications for ICU admission. This review focuses on pregnancy-specific causes of critical illness. Management of the critically ill mother poses special challenges. The physiologic changes in pregnancy and the presence of a second, dependent, patient may necessitate adjustments to therapeutic and supportive strategies. The fetus is generally robust despite maternal illness, and therapeutically what is good for the mother is generally good for the fetus. For pregnancy-induced critical illnesses, delivery of the fetus helps resolve the disease process. Prognosis following pregnancy-related critical illness is generally better than for age-matched non-pregnant critically ill patients.
Figures
Comment in
-
Critical care in pregnancy.Crit Care. 2011;15(6):1014. doi: 10.1186/cc10479. Epub 2011 Dec 22. Crit Care. 2011. PMID: 22236812 Free PMC article.
References
-
- Sriram S, Robertson MS. Critically ill obstetric patients in Australia: a retrospective audit of 8 years' experience in a tertiary intensive care unit. Crit Care Resusc. 2008;10:124. - PubMed
-
- Tang LC, Kwok AC, Wong AY, Lee YY, Sun KO, So AP. Critical care in obstetrical patients: an eight-year review. Chin Med J (Engl) 1997;110:936–941. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
