

Review
doi: 10.1016/j.clp.2011.06.013.
Controversy: antenatal steroids
Affiliations
- PMID: 21890023
- PMCID: PMC3711408
- DOI: 10.1016/j.clp.2011.06.013
Item in Clipboard
Review
Controversy: antenatal steroids
Clin Perinatol.
2011 Sep.
Abstract
There is no controversy that women at risk of preterm delivery before 32 to 34 weeks' gestational age should be treated with antenatal steroids. Three recent meta-analyses by the Cochrane Collaboration on the benefits of antenatal steroids, the choice of steroid and dosing, and repeat doses of corticosteroids comprehensively summarize the available clinical information to about 2007. However, there are many unanswered questions about which steroid and dose to use and about their use in selected populations. This review focuses on those areas of uncertainty.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
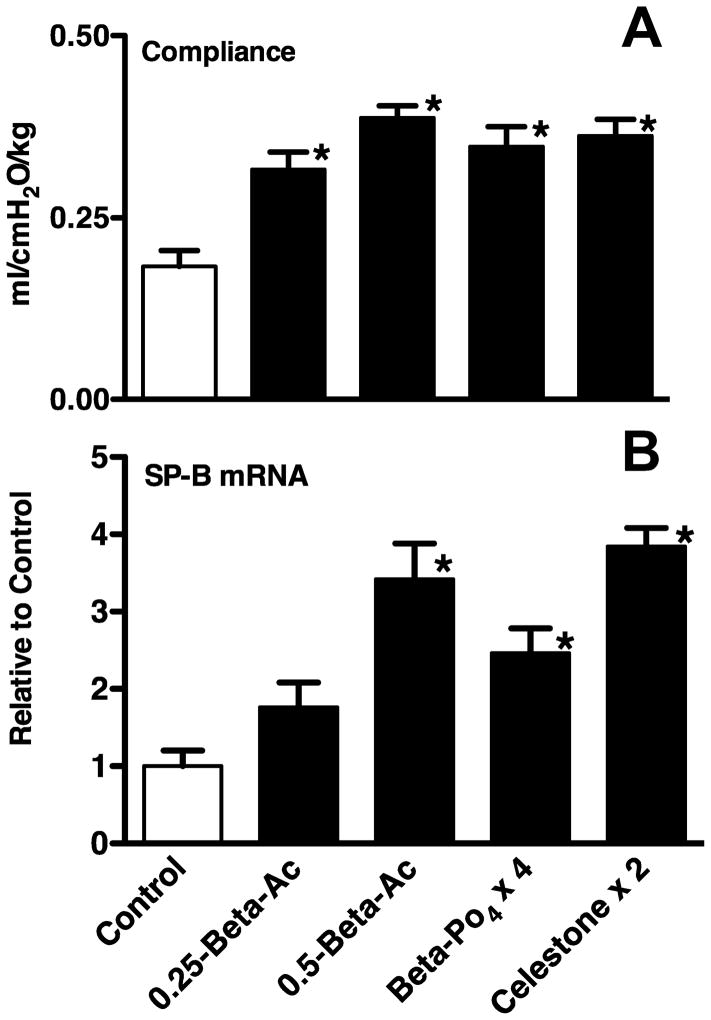
Fetal indicators of lung maturation following maternal treatments with saline (control), one dose of 0.25 mg/kg betamethasone acetate (0.25 – Beta-Ac), one dose of 0.5 mg/kg Beta-Ac, 4 doses of 0.25 mg/kg Beta phosphate (-PO4) given at 12h intervals, or 2 doses of Celestone (0.5 mg/kg of a 1 to 1 mixture of Beta Ac and Beta-PO4 given at a 24h interval). All fetuses were delivered prematurely 48h after the initial treatment. A) Lung compliance measured by the lung gas volume at 40 cmH2O pressure increased for all treated groups relative to controls. B) The mRNA for the surfactant protein (SP)-B also increased in the fetal lungs. *p<0.05 vs. controls Data from Jobe, et. al. (17).
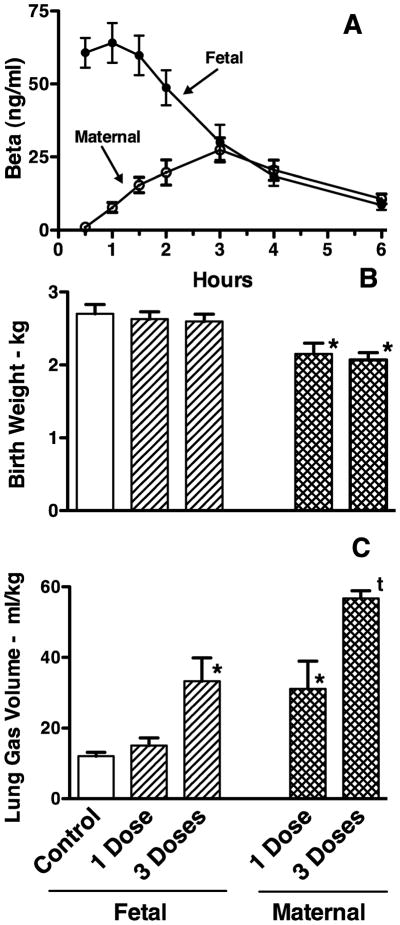
Plasma levels of betamethasone (Beta), birth weights, and lung gas volumes. A) Beta levels in fetal plasma after maternal treatments with 0.5 mg/kg Beta acetate plus phosphate (maternal) or after fetal treatment with the same dose based on estimated fetal weight (fetal). B) One or 3 weekly fetal treatments with this dose did not decrease birth weight while maternal treatments decreased birth weight. C) Lung gas volume measured at 40 cmH2O pressure as a measure of lung maturation increased more with maternal than fetal treatments. Data from Berry, et al (Frame A) (19) and Jobe, et al. (Frames B and C) (24). *p<0.05 vs. control, t p <0.05 – 3 doses maternal vs. 3 doses fetal
Similar articles
-
Incidence of respiratory disorders in neonates born between 34 and 36 weeks of gestation following exposure to antenatal corticosteroids between 24 and 34 weeks of gestation.Am J Perinatol. 2008 Feb;25(2):79-83. doi: 10.1055/s-2007-1022470. Epub 2008 Jan 10. Am J Perinatol. 2008. PMID: 18188800
-
Antenatal Corticosteroids for the Prevention of Respiratory Distress Syndrome in Premature Twins.Obstet Gynecol. 2016 Sep;128(3):583-91. doi: 10.1097/AOG.0000000000001577. Obstet Gynecol. 2016. PMID: 27500336 Clinical Trial.
-
[Value of prenatal corticotherapy in the prevention of hyaline membrane disease in premature infants. Randomized prospective study].Tunis Med. 2002 May;80(5):260-5. Tunis Med. 2002. PMID: 12534029 Clinical Trial. French.
-
Antenatal Corticosteroids: Who Should We Be Treating?Clin Perinatol. 2018 Jun;45(2):181-198. doi: 10.1016/j.clp.2018.01.002. Epub 2018 Feb 17. Clin Perinatol. 2018. PMID: 29747882 Review.
-
Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth.Cochrane Database Syst Rev. 2020 Dec 25;12(12):CD004454. doi: 10.1002/14651858.CD004454.pub4. Cochrane Database Syst Rev. 2020. PMID: 33368142 Free PMC article.
Cited by
-
Association of Antenatal Steroid Exposure With Survival Among Infants Receiving Postnatal Life Support at 22 to 25 Weeks' Gestation.JAMA Netw Open. 2018 Oct 5;1(6):e183235. doi: 10.1001/jamanetworkopen.2018.3235. JAMA Netw Open. 2018. PMID: 30646235 Free PMC article.
-
The clinical significance of a positive Amnisure test in women with preterm labor and intact membranes.J Matern Fetal Neonatal Med. 2012 Sep;25(9):1690-8. doi: 10.3109/14767058.2012.657279. Epub 2012 Apr 25. J Matern Fetal Neonatal Med. 2012. PMID: 22280400 Free PMC article.
-
Twin gestation in a septate bicornuate uterus.Case Rep Obstet Gynecol. 2012;2012:563085. doi: 10.1155/2012/563085. Epub 2012 Dec 4. Case Rep Obstet Gynecol. 2012. PMID: 23304585 Free PMC article.
-
Minireview: the impact of antenatal therapeutic synthetic glucocorticoids on the developing fetal brain.Mol Endocrinol. 2015 May;29(5):658-66. doi: 10.1210/me.2015-1042. Epub 2015 Mar 12. Mol Endocrinol. 2015. PMID: 25763611 Free PMC article. Review.
-
Counselling and management for anticipated extremely preterm birth.Paediatr Child Health. 2017 Sep;22(6):334-341. doi: 10.1093/pch/pxx058. Epub 2017 Aug 11. Paediatr Child Health. 2017. PMID: 29485138 Free PMC article.
References
-
- Crowley P, Chalmers I, Keirse MJ. The effects of corticosteroid administration before preterm delivery: an overview of the evidence from controlled trials. Br J Obstet Gynaecol. 1990;97(1):11–25. - PubMed
-
- NIH. Consensus development panel on the effect of corticosteroids for fetal maturation on perinatal outcomes. Effect of corticosteroids for fetal maturation on perinatal outcomes. J Am Med Assn. 1995;273:413–418. - PubMed
-
- Antenatal Corticosteroids Revisited: Repeat Courses. NIH Consens Statement Online 2000. 2000;17:1–10.
-
- Roberts D, Dalziel S. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006;3:CD004454. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
