

Comparison of bare-metal and drug-eluting stents in patients with chronic kidney disease (from the NHLBI Dynamic Registry)
- PMID: 21890077
- PMCID: PMC3215900
- DOI: 10.1016/j.amjcard.2011.07.029
Comparison of bare-metal and drug-eluting stents in patients with chronic kidney disease (from the NHLBI Dynamic Registry)
Abstract
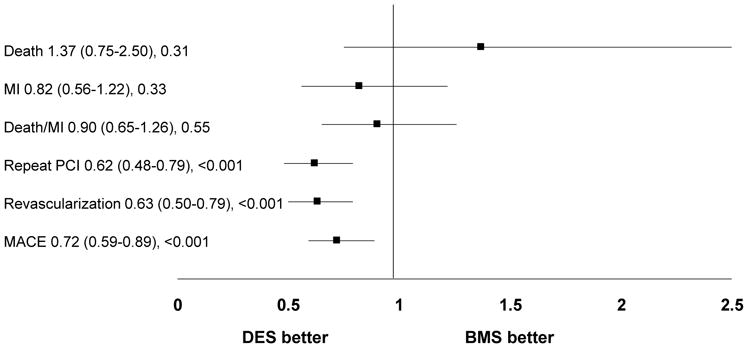
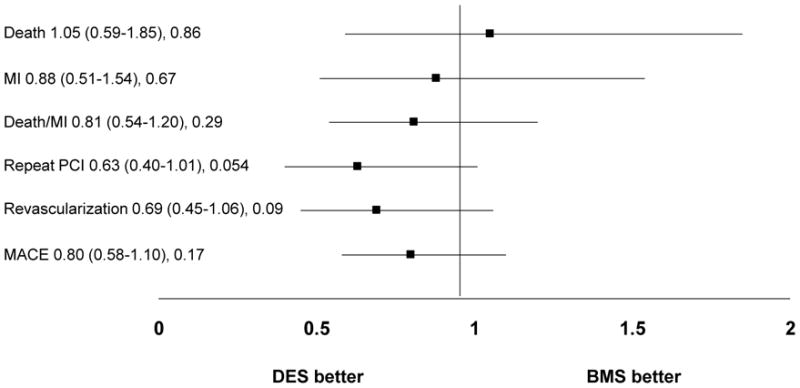
Patients with chronic kidney disease (CKD) have a disproportionate burden of coronary artery disease and commonly undergo revascularization. The role and safety of percutaneous coronary intervention (PCI) using drug-eluting stents (DESs) verses bare-metal stents in patients with CKD not on renal replacement therapy has not been fully evaluated. This study investigated the efficacy and safety of DES in patients with CKD not on renal replacement therapy. Patients were drawn from the National Heart, Lung, and Blood Institute Dynamic Registry and were stratified by renal function based on estimated glomerular filtration rate (GFR). Of the 4,157 participants, 1,108 had CKD ("low GFR" <60 ml/min/1.73 m(2)), whereas 3,049 patients had normal renal function ("normal GFR" ≥60 ml/min/1.73 m(2)). For each stratum of renal function we compared risk of death, myocardial infarction, or repeat revascularization between subjects who received DESs and bare-metal stents at the index procedure. Patients with low GFR had higher 1-year rates of death and myocardial infarction and a decreased rate of repeat revascularization compared to patients with normal GFR. Use of DESs was associated with a decreased need for repeat revascularization in the normal-GFR group (adjusted hazard ratio 0.63, 95% confidence interval 0.50 to 0.79, p <0.001) but not in the low-GFR group (hazard ratio 0.69, 95% confidence interval 0.45 to 1.06, p = 0.09). Risks of death and myocardial infarction were not different between the 2 stents in either patient population. In conclusion, presence of CKD predicted poor outcomes after PCI with high rates of mortality regardless of stent type. The effect of DES in decreasing repeat revascularization appeared to be attenuated in these patients.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–2047. - PubMed
-
- Yeo FE, Villines TC, Bucci JR, Taylor AJ, Abbott KC. Cardiovascular risk in stage 4 and 5 nephropathy. Adv Chronic Kidney Dis. 2004;11:116–133. - PubMed
-
- Al Suwaidi J, Reddan DN, Williams K, Pieper KS, Harrington RA, Califf RM, Granger CB, Ohman EM, Holmes DR., Jr Prognostic implications of abnormalities in renal function in patients with acute coronary syndromes. Circulation. 2002;106:974–980. - PubMed
-
- Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S. Renal insufficiency as a predictor of cardiovascular outcomes and the impact of ramipril: the HOPE randomized trial. Ann Intern Med. 2001;134:629–636. - PubMed
-
- Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Terirstein P, Fish D, Colombo A, Brinker J, Moses J, Shanknovich A, Hirshfeld J, Bailiey S, Elis S, Rake R, Goldberg S. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl J Med. 1994;331:496–501. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
